Having dense breast tissue is a common finding on mammograms, but it can sometimes lead to questions about cancer risk. Dense breasts can make it harder for mammograms to detect abnormalities and may be associated with a slightly higher risk of breast cancer. Understanding your breast density and how it affects your screening is important for making informed decisions about your health. Texas Breast Center, led by Dr. Gorman, is here to guide you through this process. Schedule an appointment with Texas Breast Center today for a personalized consultation.
Understanding Breast Density and What It Means for Cancer Risk
After a mammogram, patients might be informed that they have dense breasts, which can raise questions about breast cancer risk. Nearly half of women over the age of 40 have dense breast tissue, meaning their breasts contain more fibrous and glandular tissue compared to fat. This condition not only increases the risk of developing cancer, but it can also make it harder for radiologists to detect tumors on a mammogram. Dense tissue appears white on a mammogram, just like cancerous growths, making it more challenging to distinguish between the two. According to Molly Guthrie of the Susan G. Komen Breast Cancer Foundation, women with dense breasts are 4 to 5 times more likely to develop breast cancer than women without dense breasts.
The FDA has recently introduced new regulations to ensure that women are informed about their breast density following a mammogram. Understanding this information is crucial for assessing your cancer risk and determining whether additional screening may be necessary.
What Causes Dense Breasts?
Dense breast tissue is influenced by a variety of factors, including genetics and hormonal changes. The breast is composed of different types of tissue—glandular, fibrous, and fatty. Women with more glandular and fibrous tissue and less fat have denser breasts. As women age, breast density generally decreases, but some women may retain dense breast tissue throughout their lives. Breast density is not something that can be felt; it can only be determined through imaging like a mammogram.
In addition to genetic factors, dense breasts can also be influenced by lifestyle elements such as hormone replacement therapy during menopause. It’s important to remember that breast density is just one factor in cancer risk, and many women with dense breasts do not develop cancer. However, it does raise the likelihood of both developing the disease and making it harder to detect through routine mammograms.
Why Dense Breasts Make Mammograms Challenging
Dense breast tissue and tumors both appear white on a mammogram, making it difficult to detect cancer. This similarity can mask tumors and lead to a delay in diagnosis. Dr. Elizabeth Comen, a breast cancer oncologist, emphasized that this masking effect is one of the key reasons why dense breasts make detecting cancer more challenging. “When you have dense breasts, it may be harder to detect breast cancer on a mammogram, and you may need additional imaging,” she explained.
New FDA regulations now require mammography providers to notify patients of their breast density, using simpler and clearer language so that women can understand what their breast density means for their health. If you are informed that you have dense breasts, additional imaging like an ultrasound or MRI might be recommended to ensure that nothing is missed. This is especially important if you have other risk factors for breast cancer, such as family history or previous abnormal mammograms.
Does Having Dense Breasts Increase My Risk of Breast Cancer?
Yes, having dense breasts increases your risk of developing breast cancer. Research indicates that women with dense breasts are 4 to 5 times more likely to develop breast cancer than those with less dense tissue. This elevated risk stems not only from the increased likelihood of developing cancer but also from the challenge in detecting it.
However, dense breasts are just one of several factors that affect breast cancer risk. Your overall risk can be influenced by your age, family history, lifestyle choices, and genetics. It’s important to view breast density as part of the bigger picture when it comes to cancer risk. If you have dense breasts, discussing your risk profile with your doctor is essential in creating a personalized screening plan.
Additional imaging, such as ultrasounds or MRIs, can offer better detection for women with dense breasts, though these additional screenings may not always be covered by insurance. Despite this, advocates like Molly Guthrie are pushing for policy changes to make these screenings more accessible and affordable for women at higher risk.
What Should I Do If I Have Dense Breasts?
If you’ve been told that you have dense breasts after a mammogram, don’t panic. While it’s important to be aware of the increased risk, there are steps you can take to manage your health effectively:
Consult with your doctor: Discuss your overall risk factors, including family history and genetics, with your healthcare provider to develop a comprehensive plan for monitoring your breast health.
Consider supplemental imaging: Depending on your risk profile, your doctor may recommend additional screenings along with your mammogram such as an ultrasound or MRI. These screenings can provide more detailed images of dense breast tissue and help detect any hidden abnormalities.
Stay vigilant with regular mammograms: While dense breasts make detection more challenging, routine mammograms are still an essential part of breast cancer screening. Make sure to follow the recommended schedule for your age and risk category.
Lead a healthy lifestyle: Maintaining a healthy weight, exercising regularly, and avoiding smoking and excessive alcohol consumption can all help reduce your risk of developing breast cancer.
With the new FDA regulations now in effect, you’ll receive clearer guidance on your breast density and how it affects your cancer risk. Texas Breast Center, led by Dr. Gorman, is dedicated to helping patients navigate this information and create personalized screening plans that prioritize early detection.
Taking Charge of Your Breast Health
While having dense breasts increases your risk of breast cancer and makes detection more difficult, it is a manageable risk with the right screening plan. Understanding your breast density is the first step toward taking control of your breast health. With new federal regulations in place, women are now better informed about what dense breasts mean and can take appropriate action.
At Texas Breast Center, Dr. Gorman and her team are here to help you understand your individual risk and develop a screening plan tailored to your needs. If you’ve been told you have dense breasts or if you have concerns about your breast health, schedule a consultation with Dr. Gorman today.
FAQ’s About Dense Breasts on Mammogram and Breast Cancer Risk
What is the difference between dense breast tissue and adipose tissue on a mammogram?
Dense breast tissue consists of more fibrous and connective tissue, while adipose tissue is fat. Mammograms can show dense tissue as white, which makes it harder to see abnormalities like masses or tumors. Adipose tissue, on the other hand, appears dark, allowing for easier detection. At Texas Breast Center, Dr. Gorman helps patients understand their breast density and the challenges it may present in medical imaging.
Should I get a breast MRI or a breast ultrasound if I have dense breasts?
For women with dense breasts, a breast MRI or ultrasound can provide additional screening beyond a mammogram. While mammograms are the primary screening tool, these additional methods, like magnetic resonance imaging and ultrasound, may better detect cancers hidden by dense tissue. Dr. Gorman can advise on whether these exams are right for you, depending on your personal risk assessment and mammogram results.
How does the Food and Drug Administration’s regulation on dense breasts impact me?
The United States Food and Drug Administration (FDA) now requires that women be notified if they have dense breasts after a mammogram. This helps patients like you discuss appropriate next steps with healthcare providers. Texas Breast Center can help explain the notification and whether additional screening with advanced technologies may be necessary.
What is BI-RADS, and how does it relate to breast density?
BI-RADS stands for Breast Imaging-Reporting and Data System, a classification system used by radiologists to assess breast density and categorize findings from mammograms. Women with dense breasts often receive a BI-RADS score indicating they have a higher likelihood of needing additional tests. Texas Breast Center works with the BI-RADS system to give patients a clear understanding of their imaging results and the next steps.
Does having dense breasts increase my probability of needing a biopsy?
Yes, dense breasts can increase the probability of needing a biopsy due to the difficulty of distinguishing between benign and malignant masses on a mammogram. Although not all biopsies result in cancer diagnosis, Texas Breast Center, led by Dr. Gorman, uses advanced technology to ensure that any abnormalities detected in your breast imaging are properly evaluated to reduce unnecessary false positives or false negatives.
Can environmental factors influence breast density?
Yes, environmental factors like diet, exposure to certain chemicals, and medications can influence breast density, though genetics plays a larger role. For example, hormonal treatments and fatty acid intake may affect breast composition. Dr. Gorman can help assess how environmental factors might be affecting your breast health and whether changes in lifestyle or medicine may be necessary.
How does tomosynthesis help in detecting cancers in dense breasts?
Tomosynthesis, or 3D mammography, is a technology that takes multiple images of the breast from different angles. This improves the chances of detecting cancers hidden by dense connective tissue. For women with dense breasts, Dr. Gorman might recommend this advanced form of mammography, especially if past exams have resulted in unclear findings.
What is the incidence of breast cancer in women with dense breasts compared to those with fatty breasts?
The incidence of breast cancer is higher in women with dense breasts compared to those with more fatty tissue. This is because dense breasts not only increase the risk of developing cancer but also make it harder to detect. Texas Breast Center emphasizes the importance of regular screening and personalized care for women with dense breasts to stay ahead of potential risks.
Are there any specific mutations that increase the risk of cancer in dense breasts?
Yes, certain genetic mutations, like BRCA1 and BRCA2, can further increase breast cancer risk in women with dense breasts. These mutations combined with high breast density can elevate the overall risk significantly. Dr. Gorman at Texas Breast Center can provide comprehensive genetic counseling and risk assessment to determine the best screening plan for you.
Will surgery be required if dense breasts hide a tumor that develops into a neoplasm?
If a tumor (neoplasm) is detected in dense breast tissue, surgery may be an option depending on the type and stage of the cancer. While dense tissue makes tumors harder to detect early, regular exams and advanced imaging reduce the likelihood of late-stage diagnosis. Dr. Gorman at Texas Breast Center can guide you through options like surgery, biopsy, or other treatments based on the result of your imaging and overall health care plan.
When faced with a breast cancer diagnosis, one of the most difficult decisions a woman may encounter is whether to remove one or both breasts. At Texas Breast Center, we understand the weight of this decision and the importance of making a choice that aligns with your personal health needs. Our team is dedicated to providing clear, evidence-based guidance tailored to each individual. If you’re navigating this complex choice, schedule an appointment with Texas Breast Center to discuss your options with our experienced breast surgeon, Dr. Gorman.
Is Getting Both Breasts Removed Necessary or Wise?
A recent study published in JAMA Oncology by Dr. Vasily Giannakeas, Dr. David W. Lim, and Dr. Steven A. Narod delved into the long-term outcomes of various surgical treatments for unilateral breast cancer. The study, one of the largest of its kind, followed 661,270 women for up to 20 years, analyzing the effects of lumpectomy, unilateral mastectomy, and bilateral mastectomy on breast cancer mortality.
The findings were particularly insightful: while bilateral mastectomy significantly reduced the risk of developing contralateral (opposite side) breast cancer, it did not decrease the overall mortality rate from breast cancer. This outcome challenges the commonly held belief that removing both breasts can provide a survival advantage for women diagnosed with cancer in one breast. The study’s results emphasize the importance of understanding the implications of each surgical option, particularly in terms of long-term survival.
The findings from this study reinforce the importance of personalized care when it comes to breast cancer treatment. At Texas Breast Center, Dr. Gorman is dedicated to helping each patient understand the implications of their surgical options, ensuring that decisions are made with both long-term outcomes and individual needs in mind.
Why Is There No Difference in Mortality Rates Among the Surgical Options?
One of the most surprising aspects of the study is the lack of difference in breast cancer mortality rates between the different surgical groups. Whether a woman chose a lumpectomy, which is often followed by radiation therapy, unilateral mastectomy, or bilateral mastectomy, her chances of dying from breast cancer were nearly identical over the 20-year follow-up period. Specifically, the breast cancer mortality rates were 8.54% for those who underwent a lumpectomy, 9.07% for those who had a unilateral mastectomy, and 8.50% for those who chose a bilateral mastectomy.
Dr. Gorman explains that this finding highlights a crucial point: while bilateral mastectomy can reduce the risk of developing a new cancer in the other breast, it doesn’t offer a survival benefit over less extensive surgeries. The study suggests that the risk of breast cancer-related death may be more closely related to factors such as the biology of the original tumor and its potential for metastasis, rather than the presence of a new tumor in the other breast, which might require additional therapy.
What Are the Implications of This Study for Women Considering Their Surgical Options?
For women facing a breast cancer diagnosis, the decision about which surgical treatment to pursue is deeply personal and complex. The study’s findings underscore the importance of considering all aspects of breast cancer treatment, including the emotional and psychological impact of surgery, alongside the potential physical outcomes.
Dr. Gorman notes that many women choose bilateral mastectomy in the hope of reducing anxiety about future cancers and achieving a more symmetrical appearance after breast reconstruction. However, given that this approach does not appear to improve survival rates, it’s essential for patients to have a thorough discussion with their healthcare providers about the benefits and limitations of each option. This conversation should include an understanding that while bilateral mastectomy can reduce the likelihood of contralateral breast cancer, it does not eliminate the risk of breast cancer mortality.
What Is the Significance of the Study’s Contralateral Breast Cancer Findings?
The study found that women who underwent bilateral mastectomy had a significantly lower risk of developing contralateral breast cancer compared to those who had a lumpectomy or unilateral mastectomy. Specifically, the 20-year risk of developing a new cancer in the opposite breast was 6.9% in the lumpectomy and unilateral mastectomy groups, compared to just 0.3% in the bilateral mastectomy group. This suggests that removing both breasts can indeed prevent the occurrence of cancer in the other breast, but this preventive measure does not necessarily translate into a survival advantage.
While preventive mastectomy can lower the risk of developing contralateral breast cancer, this study highlights that it does not necessarily change the odds of survival. Dr. Gorman explains that these findings might seem paradoxical at first, but they point to the complex nature of breast cancer biology. The study’s authors hypothesize that the development of contralateral breast cancer may not always represent a new, independent cancer, but could instead be a manifestation of the original cancer’s metastatic potential. This theory could explain why preventing contralateral breast cancer through bilateral mastectomy does not result in better survival outcomes—because the primary concern might still be the original tumor’s ability to spread rather than the emergence of a new tumor.
What Should Patients Consider When Deciding on a Treatment Plan?
Given the study’s findings, Dr. Gorman advises that patients consider several factors when deciding on their breast cancer treatment plan. These factors include the stage and type of the original tumor, the patient’s genetic risk factors, personal preferences, and the potential impact on quality of life. It’s also essential for patients to understand that more extensive surgery does not necessarily equate to better survival outcomes.
For women with a high genetic risk, such as those with a BRCA mutation, the decision to undergo surgery may involve more complex considerations. For some women, the peace of mind that comes with bilateral mastectomy may outweigh the lack of survival benefit, and that’s a valid choice. However, for others, the knowledge that less extensive surgery can offer similar survival rates might lead them to opt for a lumpectomy or unilateral mastectomy, preserving more of their natural breast tissue and potentially reducing recovery time and surgical complications.
How Can Texas Breast Center Help You Navigate Your Options?
At Texas Breast Center, Dr. Gorman and her team are committed to providing patients with comprehensive, evidence-based information to help them make informed decisions about their breast cancer treatment. We understand that each patient’s situation is unique, and we are here to support you in choosing the option that aligns best with your health needs, lifestyle, and personal preferences.
Dr. Gorman emphasizes that the decision-making process should involve a careful evaluation of the risks and benefits of each surgical option. She and her team are dedicated to ensuring that patients fully understand the potential outcomes associated with their treatment choices, helping them feel confident and empowered in their decision.
What Is the Best Next Step?
The findings from this study offer critical insights into the complexities of breast cancer treatment. While bilateral mastectomy can effectively reduce the risk of a second cancer in the opposite breast, it does not appear to improve overall survival rates compared to lumpectomy or unilateral mastectomy. This information is crucial for women to consider as they navigate their treatment options.
If you or a loved one is facing a breast cancer diagnosis and are considering your surgical options, the team at Texas Breast Center is here to help. Schedule a consultation with Dr. Gorman today to discuss your options and determine the best course of action for your unique situation.
For more detailed information, you can access the full study here.
Breast cancer presents a significant health concern, particularly among black women, who often face higher risks and unique challenges. At Texas Breast Center, led by Dr. Gorman, we are dedicated to providing expert care and support tailored to each patient’s needs. Understanding the specific risks and proactive measures is crucial in early detection and effective treatment. Our team is committed to offering the latest advancements in breast health to our diverse community. Schedule an appointment with Texas Breast Center today to discuss your breast health and risk factors with our specialized team.
Is breast cancer risk higher among black women?
Although black women have a slightly lower incidence rate of breast cancer compared to white women, they tend to develop the disease at a younger age and are twice as likely to develop the aggressive triple-negative subtype. This aggressive form of breast cancer, combined with delayed diagnosis and treatment, contributes to black women having a 40% higher mortality rate from breast cancer than white women in the United States. Breast cancer has now become the leading cause of cancer death among black women, surpassing lung cancer, according to the American Cancer Society. The higher mortality rate underscores the importance of early detection and targeted treatment strategies for this at-risk population. At Texas Breast Center, we are dedicated to providing comprehensive care to address these specific risks and improve outcomes for black women.
Why is the breast cancer mortality rate higher among black women?
The breast cancer mortality rate is higher among black women, about 18% at five years after diagnosis, due to several key factors. Black women are more likely to be diagnosed at a later stage, with only 57% of cases found at an early stage compared to 67% in white women. They also face more aggressive tumor biology, being twice as likely to have triple-negative breast cancer and having a higher incidence of inflammatory breast cancer. Disparities in access to health care and treatment mean black women often receive lower rates of surgery and chemotherapy. Additionally, they tend to be diagnosed at younger ages, with a median age of 58 compared to 62 for white women. Genetic factors specific to African ancestry and inconsistencies in screening recommendations further contribute to the disparity. Socioeconomic barriers, experiences of medical racism, higher obesity rates, and other health issues also play significant roles. Consequently, black women have lower 5-year survival rates, with 82% living at least 5 years after diagnosis compared to 92% of white women. Addressing these disparities requires a comprehensive approach, including improved access to care, targeted screening, and continued research. At Texas Breast Center, we are committed to tackling these challenges and providing the best possible care for all our patients.
What role does genetics play in breast cancer mortality among black women?
Genetics plays a significant role in breast cancer mortality among black women, with recent research highlighting several key aspects including susceptibility to certain subtypes of breast cancer. Genetic variants specific to African ancestry have been identified, which are associated with an increased risk of developing aggressive subtypes like triple-negative breast cancer. This subtype is more challenging to treat and has a poorer prognosis, contributing to higher mortality rates. The identification of these variants has led to improved risk prediction models tailored for black women, facilitating earlier screening and intervention. Additionally, researchers have developed polygenic risk scores that combine multiple genetic variants to more accurately assess overall breast cancer risk for women of African descent.
However, genetics is not the only factor. Social and environmental factors, such as neighborhood disadvantage, also significantly impact breast cancer mortality, often interacting with genetic factors to increase the risk of aggressive tumor subtypes. While understanding genetic factors is crucial, it opens the door for more targeted screening, prevention, and treatment strategies. This underscores the need for diverse genetic studies to ensure interventions are relevant to all populations.
At Texas Breast Center, we recognize the importance of addressing both genetic and non-genetic factors to reduce breast cancer mortality rates among black women. Our approach includes comprehensive care, considering the unique genetic risks and environmental influences faced by our patients.
Are there specific genetic mutations more prevalent in black women that increase breast cancer risk?
Yes, there are specific genetic mutations more prevalent in black women that increase breast cancer risk. Research shows that black women are more likely to have mutations in the BRCA2 and PALB2 genes, which are associated with a higher risk of breast cancer, especially aggressive subtypes. Additionally, two gene variants, the ANKLE1 and Duffy gene mutations, are more common in African American women and contribute to a higher likelihood of developing triple-negative breast cancer (TNBC). The ARHGEF38 gene has also been linked to more aggressive cancer types, which are more frequent in black women.
Large-scale studies have identified genetic variants specific to women of African descent that may explain the higher incidence of aggressive breast cancer subtypes in this population. Researchers have developed polygenic risk scores that combine multiple genetic variants to provide more accurate risk assessments for black women, offering a better prediction compared to traditional methods.
While these genetic factors are crucial in understanding breast cancer risk, it is important to note that the overall rate of inherited mutations linked to breast cancer is similar between black and white women. The differences lie in the specific genes affected and the types of breast cancer associated with these mutations.
At Texas Breast Center, we emphasize the importance of understanding these genetic variations to develop more accurate risk assessment tools, improve screening protocols, and tailor prevention and treatment strategies for black women. However, genetic factors are just one piece of the puzzle, and we must also consider environmental and socioeconomic factors in determining overall breast cancer risk and outcomes.
Prioritizing Breast Cancer Care for Black Women
Understanding the unique risks and challenges that black women face with breast cancer is essential. At Texas Breast Center, our expert team is dedicated to providing personalized care that addresses these specific concerns. Early detection and targeted treatments can make a significant difference. Schedule your consultation with Texas Breast Center today and take the first step towards proactive breast health management.
FAQ’s About Breast Cancer Risk Among Black Women
What are the common symptoms of breast cancer in black women?
Common symptoms of breast cancer include a lump in the breast, changes in breast shape or size, skin dimpling, nipple discharge, or pain. Black women may experience these symptoms at a younger age and with more aggressive forms of the disease. At Texas Breast Center, Dr. Gorman and her team emphasize the importance of being aware of these symptoms and seeking medical advice promptly for early detection and treatment.
How does socioeconomic status affect breast cancer risk in black women?
Socioeconomic status can significantly impact breast cancer risk and outcomes. Limited access to healthcare, lower income, and education levels contribute to delayed diagnoses and treatments. Texas Breast Center is committed to addressing these disparities by providing accessible and comprehensive care, ensuring that every patient receives the necessary screenings and treatments regardless of their socioeconomic background.
What preventive measures can black women take to reduce their breast cancer risk?
Preventive measures include regular screenings, maintaining a healthy lifestyle, and staying informed about family history. Texas Breast Center, led by Dr. Gorman, offers tailored prevention strategies and screenings to help black women manage their breast cancer risk effectively, promoting early detection and better outcomes.
Are there lifestyle changes that can help lower breast cancer risk in black women?
Yes, lifestyle changes such as maintaining a healthy weight, eating a balanced diet, exercising regularly, limiting alcohol intake, and avoiding smoking can help lower breast cancer risk. Dr. Gorman and her team at Texas Breast Center provide personalized advice and support to help patients adopt these healthy habits, enhancing their overall breast health.
How does access to healthcare influence breast cancer outcomes for black women?
Access to healthcare plays a crucial role in breast cancer outcomes. Black women often face barriers such as lack of insurance, fewer healthcare facilities, medical bias, and economic challenges. Texas Breast Center strives to overcome these barriers by offering comprehensive and accessible care, ensuring that all women receive timely and effective breast cancer treatments.
What role do social determinants of health play in breast cancer risk for black women?
Social determinants such as income, education, neighborhood, and access to care significantly impact breast cancer risk and outcomes. Dr. Gorman and the team at Texas Breast Center recognize these challenges and are dedicated to providing holistic care that addresses both medical and social needs, helping to reduce the disparities in breast cancer outcomes.
Can genetic counseling help black women understand their breast cancer risk?
Genetic counseling can be very beneficial in understanding breast cancer risk, especially for those with a family history of the disease. Texas Breast Center offers genetic counseling services to help Black women assess their risk and make informed decisions about their health, ensuring they receive personalized and proactive care.
What are the benefits of early breast cancer screening for black women?
Early breast cancer screening, such as mammography, can lead to earlier detection, which is crucial for successful treatment and better outcomes. Dr. Gorman at Texas Breast Center emphasizes the importance of regular mammograms and other screenings, particularly for black women who are at higher risk for aggressive breast cancer types.
How can black women advocate for themselves in the healthcare system regarding breast cancer care?
Black women can advocate for themselves by being informed about their risk factors, seeking regular screenings, asking questions, and demanding timely and appropriate care. Texas Breast Center supports patient advocacy by providing education, resources, and a compassionate team led by Dr. Gorman, dedicated to empowering women to take charge of their breast health.
What support services are available for black women diagnosed with breast cancer?
Support services such as counseling, support groups, and patient education can significantly impact the journey of black women diagnosed with breast cancer. Texas Breast Center offers a range of support services designed to help patients and their families navigate the challenges of diagnosis and treatment, ensuring they receive comprehensive care and emotional support throughout their journey.
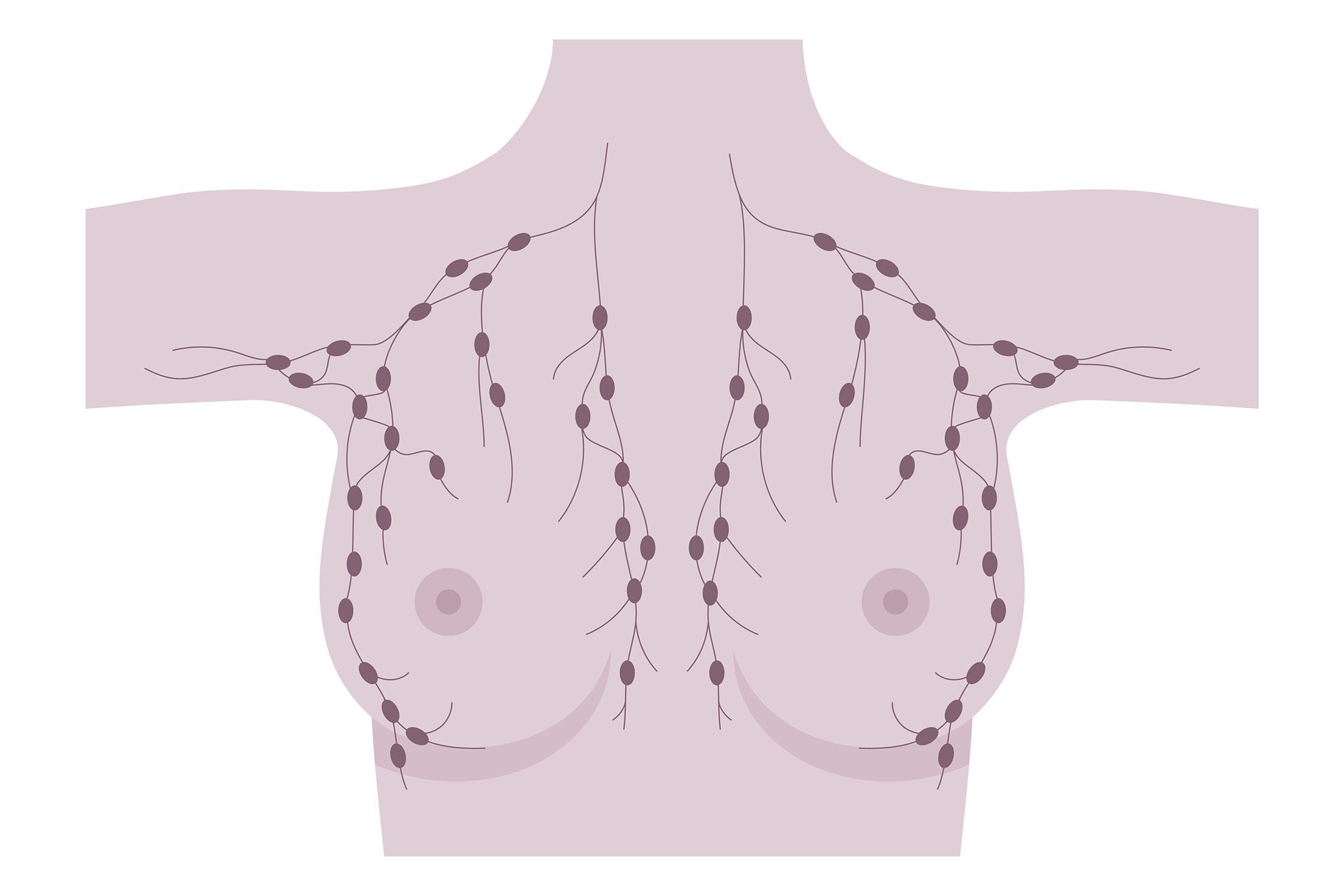
At Texas Breast Center, under the expert care of Dr. Gorman, we understand the complexities that come with a breast cancer diagnosis, including the risk of lymphedema. Breast cancer management is a multifaceted approach that addresses various complications such as lymphedema. Lymphedema, a condition of localized fluid retention and tissue swelling, can be a challenging aspect of breast cancer care. Lymphedema occurs due to the disruption of the lymphatic system, which affects lymph vessels and lymph nodes. Our team is dedicated to providing clear, straightforward information to help you manage and prevent this condition. In this article, we’ll address common questions about lymphedema and its connection to breast cancer. If you have concerns or need personalized advice, schedule an appointment with Texas Breast Center for a consultation today.
How common is lymphedema in breast cancer?
Lymphedema is a common complication following breast cancer treatment. Research indicates varying prevalence and incidence rates, with studies showing that around 30% of women treated for breast cancer experience lymphedema. Specifically, the prevalence can increase from 6.8% at baseline to nearly 24% at seven years post-diagnosis. Cumulative incidence rates reveal that lymphedema affects about 13.5% of patients at two years, 30.2% at five years, and 41.1% at ten years post-treatment.
The overall estimated incidence of chronic arm edema post-breast cancer is approximately 21.4%, with a systematic review reporting an incidence rate of 17% among survivors. Chronic arm edema is often linked to the lymphatic and blood vessels within the thorax and upper limbs. Several factors heighten the risk, including axillary lymph node dissection (ALND), radiation therapy, higher body mass index (BMI), and chemotherapy. Additionally, positive lymph node status, larger tumor size, estrogen receptor-negative breast cancer, and seroma formation after surgery are significant contributors.
Understanding these risks can help in early detection and management. Effective breast cancer management includes regular monitoring of the lymphatic system to detect early signs of lymphedema. For personalized advice and treatment options, schedule an appointment with Dr. Gorman at Texas Breast Center.
How does lymphedema impact the quality of life of breast cancer survivors?
Lymphedema involves the lymphatic system and can significantly impact the quality of life of breast cancer survivors. Physically, lymphadema can cause inflammation, pain, and reduced range of motion, affecting a woman’s daily activities. Additionally, lymphedema can cause swelling in the fingers and require the use of compression bandages and garments to manage pressure. Psychologically, it can lead to depression and anxiety. As a chronic condition, lymphedema can worsen over time if not managed properly, highlighting the importance of early intervention and continuous monitoring. Recognizing the signs and understanding the need for ongoing care are crucial for maintaining the quality of life. Dr. Gorman and the team at Texas Breast Center are dedicated to providing the comprehensive support needed to manage this condition effectively.
How can lymphedema be avoided in breast cancer?
Lymphedema, a common complication following breast cancer treatment, can be managed and potentially avoided through a combination of preventive strategies, early detection, and appropriate interventions. Dr. Gorman emphasizes minimizing axillary surgery by reducing the extent of axillary lymph node dissection (ALND), as sentinel lymph node biopsy (SLNB) is less invasive and associated with a lower risk. Avoiding extensive lymphadenectomy during breast surgery can reduce the risk of damaging lymphatic vessels and lymph nodes. Preventive lymphatic surgery, such as the lymphatic microsurgical preventing healing approach (LYMPHA), performed during ALND to connect lymphatic channels to nearby veins, can also reduce the risk of lymphedema.
Wearing compression garments, such as sleeves or bras, immediately after surgery is recommended by Dr. Gorman to help prevent fluid buildup. Compression garments apply pressure to assist in lymphatic drainage. Studies have shown that early use of compression garments can reduce the incidence of lymphedema. It is crucial to have these garments properly fitted by a specialist and to wear them as recommended, especially during activities that may increase lymphatic load.
Dr. Gorman also advocates for regular, supervised exercise programs, including strength and aerobic training, to help reduce the risk of lymphedema by promoting lymphatic flow and maintaining a healthy body weight. Specific exercises targeting the arms, shoulders, and chest, such as neck rotations, shoulder rolls, and deep breathing exercises, can be particularly beneficial. Maintaining a healthy weight through diet and exercise can significantly reduce the risk of lymphedema, as obesity is a known risk factor. Incorporating lymphatic drainage massage as part of physical therapy can also support lymph flow.
Keeping the skin clean and moisturized helps avoid complications that affect the lymph glands and vessels and prevents infections that can trigger lymphedema. Dr. Gorman advises avoiding cuts, burns, and insect bites, and promptly treating any signs of infection, such as redness or swelling, to prevent the onset of lymphedema.
Early detection through regular monitoring of limb volume and other symptoms can help catch lymphedema before it becomes severe. Techniques such as bioimpedance spectroscopy (BIS) and circumferential measurements are useful for early detection. Dr. Gorman ensures that patients are educated about the signs and symptoms of lymphedema and the importance of early intervention, empowering them with knowledge about self-care strategies. A multidisciplinary team, including surgeons, physical therapists, and lymphedema specialists, provides comprehensive care and tailored prevention strategies for patients at risk of lymphedema.
While there is no guaranteed way to completely prevent lymphedema, a combination of surgical techniques, the use of compression garments, regular exercise, weight management, and vigilant skin care can significantly reduce the risk. Early detection and a proactive approach to monitoring and managing symptoms, as recommended by Dr. Gorman, are essential for improving the quality of life for breast cancer survivors.
Take Control of Lymphedema With Texas Breast Center
Lymphedema can be a challenging complication for breast cancer survivors, but with the right strategies and support, it can be managed effectively. Dr. Gorman and the team at Texas Breast Center are committed to providing the highest level of care and expertise to help you navigate this condition. By implementing preventive measures, monitoring for early signs, and maintaining a proactive approach to management, you can significantly improve your quality of life. For personalized advice and a comprehensive care plan, reach out to Texas Breast Center and take the first step towards better health.
FAQ’s About Lymphedema and Breast Cancer
When does lymphedema start after a mastectomy?
Lymphedema can start soon after a mastectomy, with axillary surgery or lymph nodes, or it may develop months or even years later. At Texas Breast Center, Dr. Gorman advises early monitoring post-surgery to catch any signs of lymphedema early, which can help manage and mitigate symptoms effectively.
What triggers lymphedema flare-ups?
Lymphedema flare-ups can be triggered by infection, injury, or overuse of the affected limb. Dr. Gorman recommends maintaining good skin care, avoiding heavy lifting, and wearing compression garments as preventive measures to minimize the risk of flare-ups.
What are the odds of lymphedema after a mastectomy?
The odds of developing lymphedema after a mastectomy with lymph node surgery vary, but studies suggest that about 20-40% of patients may experience it. Dr. Gorman emphasizes the importance of regular follow-ups and early intervention at Texas Breast Center to reduce these odds.
What are the odds of lymphedema after a lumpectomy?
The risk of lymphedema after a lumpectomy with targeted lymph node surgery is generally lower than after a surgery with more extensive lymph node surgery, typically around 5-10%. However, Dr. Gorman and the team at Texas Breast Center still recommend vigilance and proactive measures to manage this risk.
What does breast lymphedema look like?
Breast lymphedema can cause swelling, a feeling of heaviness, and skin changes such as thickening or redness. Dr. Gorman at Texas Breast Center can provide a thorough assessment and personalized care plan to manage these symptoms effectively.
How does lymphedema make you feel?
Lymphedema can cause physical discomfort, including swelling, pain, and restricted movement, as well as emotional stress. Dr. Gorman and the team at Texas Breast Center are dedicated to supporting patients both physically and emotionally through comprehensive care.
Do compression sleeves help with lymphedema after breast cancer?
Yes, compression sleeves can be very effective in managing lymphedema by promoting lymphatic drainage and reducing swelling. Dr. Gorman advises proper fitting and regular use of compression garments, particularly during activities that may increase lymphatic load.
What can I do to reduce lymphedema?
To reduce the risk of lymphedema, follow Dr. Gorman’s recommendations: maintain a healthy weight, practice good skin care, engage in regular exercise, and use compression garments as advised. Texas Breast Center offers comprehensive guidance on these preventive strategies.
What is a lymphedema drain?
A lymphedema drain is a surgical device used to remove excess fluid buildup in the affected area. Dr. Gorman can explain the procedure and benefits of using a lymphedema drain during your consultation at Texas Breast Center to manage severe cases effectively.
Does massage help lymphedema?
Manual lymphatic drainage massage can help reduce lymphedema by encouraging the flow of lymphatic fluid through lymph vessels. Dr. Gorman often includes this as part of a comprehensive breast cancer management plan at Texas Breast Center.
Can I decline to have any lymph nodes removed with breast cancer?
While some lymph node removal, or lymphadenectomy, might be necessary to prevent the spread of cancer, Dr. Gorman will evaluate the need based on your specific case to minimize impact on the lymphatic system and reduce the risk of lymphedema.
At Texas Breast Center, we are committed to providing comprehensive care for breast cancer patients, focusing on recovery and long-term health. Exercise plays a crucial role in both recovery and reducing the risk of recurrence. Studies have shown that regular physical activity can improve physical function, reduce treatment side effects, and enhance overall well-being. Evidence from oncology research consistently supports these findings. Understanding the importance of exercise can empower patients in their recovery journey. Schedule an appointment with Texas Breast Center today for a personalized consultation on incorporating exercise into your recovery plan.
How does exercise impact breast cancer recovery and recurrence prevention?
Exercise plays a significant role in the recovery process and recurrence prevention for breast cancer survivors, in that research consistently demonstrates that engaging in regular physical activity post-diagnosis can lead to improved survival rates, better quality of life, and reduced risks of cancer recurrence. Data from cancer research and oncology studies highlight the benefits of exercise in enhancing overall prognosis.
4 Benefits of Exercise in Breast Cancer Recovery and Recurrence Prevention
Improved Survival Rates: Studies have shown that breast cancer survivors who engage in regular physical activity have a lower risk of recurrence and mortality. For instance, a meta-analysis found that exercise participation after diagnosis was associated with 34% fewer deaths from breast cancer, 41% fewer deaths from all causes, and a 24% reduction in recurrence. Another study that was done within a clinical trial found that patients meeting the minimum activity guidelines both before diagnosis and after treatment had significantly reduced risks of recurrence and mortality.
Enhanced Physical and Emotional Well-being: Regular exercise improves physical fitness, helps manage symptoms like fatigue and depression, and enhances overall quality of life. Exercise has been found to improve cardiovascular health, muscle strength, and flexibility, which are often compromised during cancer treatment.
Weight Management: Maintaining a healthy weight through exercise is crucial as obesity can increase the risk of breast cancer recurrence, especially after menopause. Exercise helps in managing body weight and reducing fat, which is linked to lower estrogen levels and reduced cancer risk.
Lymphedema Management: Engaging in prescribed exercise, especially resistance training, has been shown to help manage or even prevent lymphedema, a common side effect of breast cancer treatment involving swelling in the arms.
What are the exercise recommendations for breast cancer survivors?
The American College of Sports Medicine as well as the American Cancer Society recommend the following for breast cancer survivors:
Aerobic Exercise: At least 150 minutes of moderate-intensity aerobic exercise or 75 minutes of vigorous-intensity aerobic exercise per week. Activities can include walking, cycling, swimming, or using aerobic equipment.
Resistance Training: Strength training exercises at least two days per week, focusing on major muscle groups. This helps in rebuilding muscle strength lost during treatment and managing body weight.
Flexibility and Balance Exercises: Activities like yoga and Pilates are recommended to improve flexibility, balance, and overall physical function, which can be beneficial especially after surgery or during recovery.
Are there any safety precautions when it comes to exercise for breast cancer survivors?
Yes, there are safety precautions for breast cancer survivors when it comes to exercise. Exercise programs should be tailored to individual capabilities and recovery stages, starting slowly and gradually increasing intensity and duration. Before beginning any exercise regimen, survivors should consult their healthcare providers to ensure the activities are safe, especially if there are complications like bone metastasis or low immunity. Monitoring for adverse effects such as increased pain, fatigue, or lymphedema is crucial, and exercise programs should be adjusted accordingly. At Texas Breast Center, we prioritize personalized and safe exercise plans to support our patients’ recovery.
How soon after breast cancer treatment should exercise be incorporated into a recovery plan?
Incorporating exercise into a recovery plan after breast cancer treatment should be based on individual health status, the type of treatment received, and specific recommendations from healthcare providers. Generally, starting with gentle activities as soon as it is safe can be beneficial for recovery.
Immediate Post-Treatment Period: For many patients, light physical activity such as walking can begin almost immediately after surgery, depending on the individual’s condition and the extent of the surgery. Healthcare providers often encourage gentle walking to help reduce the risk of blood clots and improve circulation.
Exercise After Surgery: Specific exercises aimed at regaining shoulder and arm mobility can usually begin within a few days post-surgery, unless contraindicated by the surgical team. These exercises are crucial for preventing stiffness and maintaining range of motion. Patients are generally advised to start with gentle stretches and gradually increase their activity level as tolerated.
During Chemotherapy and Radiation: Exercise during chemotherapy and radiation is still possible and beneficial but should be adjusted according to energy levels and side effects. Low-impact activities like walking, yoga, and gentle stretching are often recommended. It is important to avoid public gyms if the immune system is compromised due to chemotherapy. Swimming might be restricted during certain treatments to avoid infections and irritation from chlorine.
Long-Term Recovery: After completing major treatments like surgery, chemotherapy, or radiation, the intensity and amount of exercise can gradually increase. The American College of Sports Medicine and other health organizations recommend at least 150 minutes of moderate aerobic exercise per week, strength training exercises for major muscle groups at least twice a week, and flexibility exercises. These activities help improve overall physical function, reduce fatigue, and potentially decrease the risk of cancer recurrence.
Consultation with Healthcare Providers: Before starting any exercise program, it is crucial for breast cancer survivors to consult with their healthcare team. This ensures that the exercise program is safe and appropriately tailored to their specific medical conditions and recovery stage. For instance, patients with lymph node removal should get specific guidance to reduce the risk of lymphedema.
Incorporating exercise into a recovery plan after breast cancer treatment should be a gradual process tailored to the individual’s health status and treatment phase. Starting with gentle activities soon after treatment and progressively increasing the intensity as tolerated can aid in recovery and improve long-term health outcomes. Always consult with healthcare providers to tailor the exercise plan appropriately.
Take Charge of Your Recovery with Exercise
Incorporating exercise into your breast cancer recovery plan can make a significant difference in your long-term health and well-being. At Texas Breast Center, we provide personalized guidance to help you safely and effectively integrate physical activity into your routine. Our expert team is here to support you every step of the way. Schedule an appointment with Texas Breast Center today to create a customized exercise plan that fits your recovery journey.
FAQ’s About Impact of Exercise on Breast Cancer Recovery and Recurrence Prevention
Can exercise reduce the risk of breast cancer recurrence?
Yes, regular exercise can significantly reduce the risk of breast cancer recurrence. Studies show that physical activity can decrease the likelihood of cancer returning by improving immune function and reducing inflammation. Data from various cancer research studies support this. At Texas Breast Center, we tailor exercise recommendations to each patient’s medical diagnosis to maximize these benefits.
What types of exercise are best for breast cancer recovery?
A combination of aerobic exercise, strength training, and flexibility exercises is ideal. Activities like walking, swimming, resistance training, and yoga help improve overall physical function and well-being. Exercise also promotes a healthy diet and overall lifestyle, which are crucial for recovery. Texas Breast Center offers personalized exercise plans as a preventive healthcare tool to ensure each patient gets the most suitable and effective workout regimen.
How does exercise help with the side effects of breast cancer treatment?
Exercise can alleviate many treatment-related side effects such as fatigue, pain, and depression. It enhances cardiovascular health, muscle strength, and mental well-being, contributing to a better quality of life. Physical therapy, combined with a healthy diet, can also play a significant role in managing these side effects. Texas Breast Center emphasizes incorporating exercise to help manage these side effects effectively.
Is it safe to exercise during breast cancer treatment?
Yes, but exercise intensity and type should be adjusted based on treatment phase and individual health. Light activities like walking or yoga can be beneficial even during treatment. Consulting with healthcare providers ensures the exercise regimen is safe, especially for those with chronic conditions or undergoing hormone therapy. Texas Breast Center provides guidance to ensure exercises are safe and effective for each patient’s condition.
How does exercise impact survival rates in breast cancer patients?
Exercise has been shown to improve survival rates by enhancing overall health and reducing cancer-related fatigue and other symptoms. Patients who engage in regular physical activity tend to have better outcomes. Evidence from systematic reviews and clinical studies supports these findings. Texas Breast Center supports integrating exercise into recovery plans to help improve survival rates and overall prognosis.
Can exercise help with lymphedema management?
Yes, exercise, particularly resistance training, can help manage and prevent lymphedema. It improves lymphatic flow and reduces swelling. Incorporating physical therapy and exercises that target skeletal muscle can be particularly beneficial. Texas Breast Center offers specific exercise recommendations to address lymphedema, helping patients manage this common side effect of breast cancer treatment.
How does exercise affect mental health during breast cancer recovery?
Exercise positively impacts mental health by reducing symptoms of anxiety and depression, enhancing mood, and boosting self-esteem. Regular physical activity promotes the release of endorphins, which improve mental well-being and help manage stress. Knowledge of these benefits can motivate patients to stay active. Texas Breast Center includes mental health benefits as a key component of exercise plans for recovery.
What role does exercise play in weight management after breast cancer treatment?
Maintaining a healthy weight is crucial, as obesity can increase the risk of cancer recurrence. Exercise helps manage body weight and reduces fat, contributing to lower estrogen levels and reduced cancer risk. Dieting and proper nutrition also play significant roles in weight management. Texas Breast Center integrates weight management strategies, including diet and exercise, into their exercise recommendations.
Are there specific exercises to avoid during breast cancer recovery?
Certain high-impact or strenuous activities might need to be avoided, especially if there are complications like bone metastasis. It’s essential to consult healthcare providers to determine safe exercises, particularly for those with chronic conditions. Texas Breast Center customizes exercise plans to avoid any activities that could be harmful while focusing on safe and effective recovery strategies.
How soon can I start exercising after completing breast cancer treatment?
The timing for starting exercise varies based on individual health and treatment type. Generally, light activities can begin soon after treatment, with intensity gradually increasing over time. Monitoring signs and symptoms is crucial to avoid overexertion. Texas Breast Center helps patients determine the optimal time to start and progressively increase their exercise regimen for safe and effective recovery.
Facing breast cancer is challenging, and understanding the side effects of its treatment is crucial for patients. At Texas Breast Center, we recognize the importance of addressing concerns, including the potential onset of menopause due to cancer therapies. Our dedicated team is here to guide you through each step, providing clarity and support. For personalized advice and a thorough evaluation of your treatment options, we encourage you to schedule an appointment with Dr. Gorman at Texas Breast Center today.
Will I go into menopause as a result of my breast cancer treatment?
It is possible to enter menopause as a result of breast cancer treatment. Various treatments, like chemotherapy and hormone therapy, can trigger menopausal symptoms or actual menopause, with effects varying based on the patient’s age and health.
According to a study in The Journal of the Menopause Society, 56.0% of women reported one or more menopausal symptoms during the first 6 months after breast cancer diagnosis, regardless of their menopausal status at the time of diagnosis. The study also found that chemotherapy was positively associated with the occurrence of menopausal symptoms, particularly in premenopausal women.
The same study also reports that chemotherapy-induced menopause occurred in:
31% younger than 40.
53% aged 40-50.
83% aged 50+ years.
Hormone receptor-positive breast tumors often require hormonal therapies that can affect the menstrual cycle, especially in premenopausal women, leading to low estrogen levels and symptoms that mimic menopause. Chemotherapy, especially in older women, may cause a permanent end to menstruation. Drugs like tamoxifen and aromatase inhibitors, while treating breast cancer, can also induce menopausal symptoms, and contraception may still be necessary to prevent pregnancy during this time. Additionally, surgical or medically-induced ovarian suppression can lead to menopause, with the possibility of severe and sudden symptoms.
Chemotherapy works by targeting fast-dividing cells, including those in the ovaries, potentially leading to menopause. The impact of chemotherapy on menopause depends significantly on the patient’s age and the specific chemotherapy drugs and dosages used. Surgery to remove the ovaries, often considered by those at high genetic risk for breast cancer, results in immediate and permanent menopause.
Ovarian shutdown or suppression through medication can be a strategy to preserve fertility for pre-menopausal women undergoing treatment, with the potential for ovarian function to resume post-treatment. Hormonal therapy for hormone receptor-positive breast cancer, while not directly causing menopause, can result in menopausal symptoms due to its mechanism of lowering estrogen levels or blocking its effects on cancer cells.
Understanding the intricate relationship between breast cancer treatment and menopause is crucial. At Texas Breast Center, we prioritize informed discussions with our patients about these potential changes, offering guidance on managing symptoms and considering fertility preservation where applicable.
What are the symptoms of menopause I might experience after breast cancer treatment?
After breast cancer treatment at Texas Breast Center, you may experience various menopausal symptoms due to decreased sex hormone levels include physical, cognitive, and sexual symptoms. These symptoms, similar to natural menopause but often more sudden and severe, can range from hot flashes and night sweats to mood swings and cognitive challenges like memory lapses and concentration difficulties, often referred to as “brain fog.” Physical discomforts may include joint and muscle pain, potentially leading to osteoporosis, as well as headaches and changes in sexual health, such as reduced libido, vaginal dryness, and urinary issues. Women may also experience increased anxiety, perspiration, sleep disturbances, and sexual dysfunction, including dyspareunia and xeroderma (dry skin), due to the changes in the endocrine system after menopause.
The intensity and mix of signs and symptoms of menopause differ among individuals, with factors like the type of breast cancer treatment playing a significant role. Treatments like chemotherapy, hormone therapy, and ovarian suppression can lead to a range of effects, from vaginal and urinary changes to emotional and cognitive fluctuations. Managing these symptoms effectively involves a personalized approach, considering each patient’s specific needs and medical background.
At Texas Breast Center, Dr. Gorman understands the complex interplay of menopause and breast cancer treatment. Our commitment is to provide comprehensive care and support, helping you navigate these changes with tailored strategies to alleviate symptoms and improve quality of life.
What can I do to relieve symptoms of menopause after breast cancer treatment?
To alleviate menopause symptoms after breast cancer treatment, several strategies can be considered, focusing on lifestyle changes, non-hormonal medications, and complementary therapies. Maintaining a healthy weight and regular exercise can mitigate symptoms like hot flashes, while avoiding trigger foods such as spicy dishes may also provide relief. Non-hormonal medications, including certain antidepressants and gabapentin, have shown efficacy in reducing hot flashes. Complementary therapies like acupuncture and cognitive behavioral therapy offer additional support for symptom management.
Addressing vaginal dryness involves non-hormonal moisturizers and vaginal lubrication, with potential discussions about low-dose hormonal treatments or newer techniques like vaginal tissue rejuvenation. For overall bone health, especially to counteract potential osteoporosis, monitoring and possibly supplementing with vitamin D and calcium is often advised. Venlafaxine, an enzyme inhibitor, is often prescribed to manage hot flashes, which are frequent and intense perspirations commonly experienced during menopause.
It’s critical to avoid hormone replacement therapy (HRT) due to the increased risk of cancer recurrence in breast cancer survivors. Venlafaxine, an enzyme inhibitor, is often prescribed to manage hot flashes, which are frequent and intense perspirations commonly experienced during menopause. Regular communication with healthcare providers like Dr. Gorman at Texas Breast Center is essential to tailor a safe and effective breast cancer management plan for menopause symptoms post-breast cancer treatment, ensuring it aligns with the patient’s specific health history and current condition.
Navigating Menopause After Breast Cancer
Menopause following breast cancer treatment can be a complex and individual experience. At Texas Breast Center, Dr. Gorman and our team are dedicated to supporting you through this transition. We provide personalized care plans to manage menopausal symptoms effectively and improve your quality of life. If you’re navigating menopause as a result of breast cancer treatment, don’t face it alone. Contact Texas Breast Center to schedule a consultation with Dr. Gorman. Together, we can find the best approach to manage your symptoms and support your overall well-being.
More FAQ’s About Menopause As A Result Of Breast Cancer Treatment
What is the likelihood of experiencing menopause after breast cancer treatment?
The likelihood varies depending on age, type of treatment, and individual health. Texas Breast Center can provide a personalized assessment based on your specific circumstances and treatment plan.
Can menopause induced by breast cancer treatment be reversed?
Induced menopause can be permanent or temporary, especially after chemotherapy. Texas Breast Center offers guidance on managing both temporary and permanent menopause post-treatment.
Are menopausal symptoms after breast cancer treatment different from natural menopause?
Symptoms can be similar, but often more severe or abrupt after treatment. Texas Breast Center helps manage these symptoms, offering tailored support and treatment options.
How does hormone therapy for breast cancer affect menopausal symptoms?
Hormone therapy can exacerbate menopausal symptoms due to estrogen level changes. Texas Breast Center provides strategies to mitigate these effects and improve comfort.
Can breast cancer treatment-induced menopause affect my sexual health?
Yes, it can lead to vaginal dryness, discomfort, and libido changes. Texas Breast Center addresses these concerns with appropriate non-hormonal treatments and counseling.
What lifestyle changes can help manage menopause symptoms after breast cancer treatment?
A healthy diet, regular exercise, and stress reduction can alleviate symptoms. Limiting alcohol intake is recommended as it can affect the frequency and intensity of menopausal symptoms. Additionally, women who are nursing should consult with their medicine provider for personalized advice. Texas Breast Center offers lifestyle advice and support to navigate these changes effectively.
Is it safe to take hormone replacement therapy (HRT) for menopause symptoms after breast cancer treatment?
HRT is generally not recommended due to the risk of cancer recurrence. Texas Breast Center explores safer alternatives to manage menopausal symptoms post-treatment.
How can I protect my bone health during menopause after breast cancer treatment?
Regular monitoring and supplements like calcium and vitamin D are crucial. Texas Breast Center provides comprehensive care for bone health during menopause.
Will my menopause symptoms after breast cancer treatment ever improve or go away?
Symptoms may lessen over time, but individual experiences vary. Texas Breast Center monitors and adjusts treatment plans to maximize symptom relief.
Can breast cancer treatments directly cause menopause, or do they just bring on symptoms?
Some treatments, especially chemotherapy and ovarian suppression, can cause actual menopause, not just symptoms. Texas Breast Center can help distinguish and manage both scenarios.
How does feminizing hormone therapy impact women with a BRCA gene mutation and hormone receptor-positive breast cancer?
At Texas Breast Center, feminizing hormone therapy is carefully considered for patients with BRCA gene mutations and hormone receptor-positive breast tumors. The therapy can influence the risk of ovarian cancer, and medical diagnosis and treatments are tailored to ensure safety and efficacy in the United States.
Breast cancer – a term that evokes a myriad of emotions. Fear, anxiety, uncertainty, and hope are just a few that surge within countless women and their loved ones every year. We get it. It’s daunting to think of a potential diagnosis and even more challenging to navigate the complex maze of medical testing and evaluations. With rapidly evolving research and innovative developments, Advanced Breast Cancer Testing has become more sophisticated and intricate than ever before. New advancements like circulating tumor DNA analysis, the groundbreaking work on the CERIANNA PET scan, and the ever-promising liquid biopsy study are making waves in the medical community. However, for someone seeking clarity and answers, it can sometimes feel overwhelming.
Dr. Valerie J. Gorman, the esteemed founder of Texas Breast Center, understands this deeply. She recognizes the plethora of questions, apprehensions, and aspirations you hold. What does this test mean? How will it affect my treatment? Am I getting the best care possible? At Texas Breast Center, we want to assure you – you are not alone in this journey. We are here to help you understand each procedure and every result and to walk with you every step of the way. Our mission is clear: to offer an advanced, personalized, and targeted approach to breast surgery and the treatment of breast cancer. But beyond the cutting-edge medical practices and protocols lies a team genuinely devoted to the well-being of each patient.
Advanced Breast Cancer Testing is a beacon of hope in the realm of oncology and breast health. It provides a more detailed, nuanced, and comprehensive understanding of breast cancer, enabling medical professionals to tailor treatments more effectively. Yet, the journey, with its highs and lows, can be intense. It’s a path filled with questions, hopes, fears, and discoveries. At Texas Breast Center, we understand this intimately. With radical empathy, world-class expertise, and a patient-first approach, we are here to guide, support, and stand with you, ensuring that your journey is met with the best care and understanding possible.
Advancements in Breast Cancer Testing: Pioneering the Future of Breast Health
Breast cancer is not just one disease but an array of different types of cancer, each with its unique challenges and treatment approaches. Recognizing these nuances, the field of breast cancer research and diagnosis has witnessed groundbreaking advancements in recent years. At the heart of these advancements is the commitment to early detection, precise diagnosis, and tailored treatments, ensuring the best possible health outcomes for patients.
Circulating Tumor DNA (ctDNA)
One of the most promising advancements is the study of circulating tumor DNA, often referred to as ctDNA. As cancer cells, including breast cancer cells, grow and multiply, they release tiny fragments of their DNA into the bloodstream. By analyzing this DNA through blood tests, physicians can gather essential information about the tumor, including its type, genetic mutations, and potential resistance to therapies. Such detailed pictures of the cancer enable health care providers, like Dr. Valerie Gorman at Texas Breast Center, to prescribe personalized treatment plans, optimizing the chances of success while minimizing side effects.
Chemotherapy Personalization
Chemotherapy has been a cornerstone in the treatment of cancer. However, the side effects and the strain it puts on a patient’s quality of life have always been concerns. The latest advancements now allow for testing to determine the specific type of chemotherapy a patient might need, if any at all. This means that chemotherapy can be targeted, reducing unnecessary treatments and ensuring patients receive only what’s beneficial for their particular cancer type.
CERIANNA PET Scan
The CERIANNA PET scan represents a significant leap in imaging tests, especially for those with estrogen-receptor-positive breast cancer. Unlike traditional mammography or MRI, this PET scan uses a radioactive form of estrogen to detect and image hormone-dependent cancers. Dr. Gorman, always at the forefront of oncology advancements, believes in the power of such innovative medical imaging methods to enhance the accuracy of breast cancer diagnosis.
Liquid Biopsy Studies
The liquid biopsy is another transformative advancement in the world of breast cancer screening. Unlike traditional biopsies that require tissue sampling through invasive procedures, liquid biopsies detect cancer through a simple blood test. This test screens for ctDNA, providing information on potential cancer long before symptoms or signs become apparent. The implications of this are vast, offering the possibility of diagnosing breast cancer at an even earlier stage, improving the chances of successful treatment and boosting survival rates. The studies surrounding liquid biopsies are still ongoing, but the potential they hold is undeniable.
At Texas Breast Center, under the leadership and expertise of Dr. Gorman, these advancements aren’t just seen as medical breakthroughs but as vital tools to enhance patient care. Every breast self-examination, every mammogram, every breast MRI, and each piece of research brings with it a hope to improve the lives of countless women, ensuring they receive the most advanced, personalized, and compassionate care possible. With a commitment to staying updated with the latest in breast health and an unending dedication to her patients, Dr. Gorman and her team continue to lead the way in breast cancer management.
Breast cancer, with all its complexities and challenges, requires a multi-faceted approach. With these advancements, physicians can not only diagnose and treat breast cancer more effectively but also provide patients with a clearer understanding and a brighter outlook. In this journey, Texas Breast Center stands as a beacon, combining the best of technology, research, and human touch, ensuring that every patient feels seen, understood, and cared for.
Why Texas Breast Center is the Best Choice for Advanced Breast Cancer Testing
Navigating the journey of breast cancer screening, diagnosis, and treatment is undeniably complex. In this critical path, choosing the right health care provider can make all the difference. Enter Texas Breast Center, a beacon of excellence in the realm of breast health, led by the distinguished Dr. Valerie Gorman. Here’s why choosing Texas Breast Center for your Advanced Breast Cancer Testing is an informed and empowering decision:
Expertise and Experience: Dr. Gorman isn’t just a breast surgeon; she’s a specialist in surgical oncology and surgical diseases of the breast. Board certified by the American Board of Surgery, Dr. Gorman’s expertise ensures that every mammography, breast MRI, breast ultrasound, and biopsy is conducted and interpreted with utmost precision. Her extensive experience, combined with her role as Chief of Surgery and Medical Director of Surgical Services at Baylor Scott & White Medical Center – Waxahachie, ensures that patients receive world-class care.
Comprehensive Screening Options: Breast cancer isn’t a one-size-fits-all disease. Texas Breast Center recognizes this and offers a broad spectrum of screening tests, from traditional mammography in women to advanced imaging tests like the breast magnetic resonance imaging (MRI). Furthermore, for those with dense breasts, the center offers digital breast tomosynthesis, providing more detailed pictures and reducing the chances of false positives and false negatives.
Personalized Approach: Every woman’s journey and risk factors are unique. Whether you have a family history of breast cancer, carry the BRCA1 or BRCA2 gene mutation, or are simply practicing preventive healthcare, Texas Breast Center tailors its approach to fit your needs. Through self-awareness initiatives like breast self-examination and more advanced procedures like genetic testing, Dr. Gorman and her team ensure that your screening aligns with your personal risk and concerns.
Cutting-Edge Technology: Staying at the forefront of medical advancements, Texas Breast Center employs the latest technologies and research in their screenings. From exploring the potentials of liquid biopsy to utilizing the innovative CERIANNA PET scan for estrogen-receptor-positive cases, the center ensures that patients benefit from the very best the medical world has to offer.
Patient-Centered Care: Beyond the technology and expertise, what truly sets Texas Breast Center apart is its radical empathy and commitment to patient well-being. Understanding the anxiety and concerns surrounding breast cancer screening and diagnosis, Dr. Gorman and her team prioritize patient comfort, clarity, and emotional support. From assisting with health insurance plans to addressing concerns about radiation therapy or hormone therapy, every step is taken with the patient’s holistic well-being in mind.
Collaborative Research and Partnerships: Texas Breast Center isn’t just a treatment facility; it’s a hub of learning and research. Collaborating with institutions like the National Cancer Institute and American Cancer Society, the center is always at the pulse of the latest in oncology research. This ensures that patients have access to the latest treatments, therapies, and clinical trials.
Comprehensive Post-Diagnosis Care: Should a patient’s test results indicate the presence of cancer cells, the journey doesn’t end with a diagnosis. From advanced cancer staging to tailored breast cancer management plans, Dr. Gorman’s comprehensive approach ensures that patients are supported throughout their treatment, whether it involves surgery like mastectomy, radiation therapy, or targeted drug therapies.
Texas Breast Center, under the guidance of Dr. Gorman, stands out as a paradigm of excellence in breast health. With a fusion of advanced technology, medical expertise, and a heartfelt commitment to patient care, it truly is the best choice for those seeking clarity, comfort, and the best possible outcomes in their breast cancer journey.
Artificial Intelligence (AI) and Mammograms: Enhancing Diagnostic Precision
Mammograms are an essential tool in breast cancer screening, offering a detailed insight into the intricate layers of breast tissue. Traditional mammography has always depended on the expertise and vigilance of radiologists, who sift through each image, identifying even the most subtle indications of abnormalities. Yet, even the keenest human gaze can sometimes overlook nuances, leading to both false positives and false negatives. Data suggests that nearly 49% of individuals undergoing mammograms annually over a span of ten years may encounter a false positive result, while between 10% and 30% face a false negative.
Enter the revolutionary realm of Artificial Intelligence (AI). This technological advancement promises to augment the landscape of medical imaging, especially in mammography. While Texas Breast Center, led by the esteemed Dr. Valerie Gorman, has always embraced innovation, the potential integration of AI with mammogram practices has generated palpable excitement.
AI’s Role in Enhancing Mammography:
When one thinks of AI, it might bring to mind images of complex machinery or cutting-edge software. However, in the context of mammography, it’s about magnifying precision and augmenting the radiologist’s discernment. AI software, constructed on intricate algorithms, quickly assesses mammogram images, pinpointing areas that may be of concern. These areas might represent dense breast tissue, calcifications, or other subtle indications of potential breast disease or cancer.
Complementing, Not Replacing Human Expertise:
It’s crucial to note that while AI offers an additional layer of analysis to mammograms, it’s not here to replace invaluable human expertise. Research indicates that AI, in its current evolution, isn’t quite ready to operate without the discerning eye of a radiologist. The harmony of AI algorithms combined with human judgment could potentially elevate the accuracy of mammography readings.
While Texas Breast Center continually strives to offer the best in patient care, the prospect of incorporating AI into mammography has been met with optimism. Dr. Gorman and her team recognize the potential advantages and look forward to a future where technology and human expertise meld seamlessly, ensuring patients receive the most thorough analysis.
The Prospective Integration of AI at Texas Breast Center:
While AI’s full integration into mammogram readings is still on the horizon, Texas Breast Center is poised and ready for the advancements the future holds. In partnership with esteemed organizations like the American Cancer Society and the National Cancer Institute, Dr. Gorman actively participates in studies that explore the perfect blend of artificial and human intelligence in breast cancer diagnosis and treatment. The ultimate goal is clear: every patient should benefit from the unparalleled accuracy this union promises, reducing the anxieties associated with false results.
The potential of AI in mammography isn’t just about adopting a new technology. For Texas Breast Center, it represents an exciting future direction, one that prioritizes patient care, peace of mind, and a commitment to ensuring each breast health journey is marked by excellence in both technology and human touch.
Navigating the Path Ahead with Understanding and Precision
Navigating the complexities of breast health, from understanding the signs and symptoms to choosing the most appropriate screening tests, can be daunting. However, with medical advancements like artificial intelligence aiding mammography and a plethora of research from institutions like the National Cancer Institute, the future looks promising. The goal is clear: early detection, accurate diagnosis, and effective treatment of breast cancer.
Dr. Valerie Gorman has always championed a patient-centric approach. Recognized for her expertise in surgical oncology, Dr. Gorman is well-versed in the nuances of breast disease, breast cancer management, and the various stages of breast cancer. Her commitment is to ensure that every patient, whether at average risk or high risk, benefits from personalized care, cutting-edge medical imaging, and the most informed treatment choices.
As breast self-examination, mammography, and breast MRI remain pivotal in breast cancer screening, Texas Breast Center’s interest in emerging technologies like Circulating Tumor DNA (ctDNA), the CERIANNA PET scan, liquid biopsy, personalized chemotherapy, and AI signifies its forward-thinking approach. Texas Breast Center aims to offer comprehensive care, encompassing everything from genetic testing to hormone therapy, radiation therapy, and surgery, ensuring that patients are supported at every phase of their breast health journey.
Prioritize Your Breast Health with Texas Breast Center
If you or a family member has concerns about breast health, breast density, or if you’re seeking more information on breast cancer screening recommendations, don’t hesitate to reach out to Texas Breast Center. Let Dr. Gorman and her team be your trusted partners, empowering you with knowledge, compassion, and the best that medical science has to offer.
Remember, your breast health journey doesn’t have to be taken alone. With the right information, proactive screenings, and a dedicated team by your side, you can confidently navigate any challenges that come your way. Schedule a consultation today and invest in a future of optimal breast health.
More FAQ’s About Advanced Breast Cancer Testing
What are the signs and symptoms of breast cancer?
The most common symptom of breast cancer is a breast mass or lump. Other symptoms include changes in breast skin, pain, nipple discharge, and swelling in the lymph nodes of the axilla (armpit). Regular breast exams help in early detection.
Why is it essential to get a medical diagnosis if I find a breast mass or any changes in my breast?
A medical diagnosis helps identify the type of breast change, whether it’s a neoplasm, benign condition, or carcinoma in situ like ductal carcinoma. Dr. Gorman at Texas Breast Center uses advanced techniques for accurate diagnosis, guiding your next steps.
How does a breast X-ray or mammogram help in detecting breast cancer?
A mammogram uses ionizing radiation to create detailed images of the breast, helping radiology experts find breast cancer early before any symptoms appear. Dr. Gorman emphasizes the importance of regular screening mammography, especially for women at average risk.
Is there a concern about overdiagnosis with breast cancer screening tests?
Overdiagnosis refers to detecting cancers that would not have caused harm during a woman’s lifetime. While there’s a possibility of overdiagnosis, Dr. Gorman believes that the benefits of finding breast cancer early and reducing the risk of advance cancer outweigh the harms of screening.
I’ve heard of false positive results and false negative test results in mammograms. Can you explain?
A false positive test result indicates abnormalities that could be cancer when there isn’t any, leading to more tests and possibly stress. A false negative test result misses a cancer that’s present. Combining other tests, like a diagnostic mammogram or breast imaging, with a clinical breast exam can reduce type I and type II errors. Dr. Gorman ensures comprehensive screening to minimize these errors.
What is the recommended starting age for breast cancer screening?
Screening recommendations can vary, but many health professionals, including obstetricians and gynecologists, suggest starting at age 40 for most women. However, women with a strong family history or genetic risks like BRCA mutation might begin screening at a younger age. Discuss your personal risk with Dr. Gorman for a tailored recommendation.
Are there genetic tests to determine breast cancer risk?
Yes, genetic tests like those for BRCA mutations can identify women at increased risk for breast and ovarian cancer. Dr. Gorman offers comprehensive breast cancer risk assessment, including genetic testing and counseling, to guide your preventive measures.
What happens after a positive screening mammogram?
If there are abnormal findings in a screening mammogram, follow-up tests like a diagnostic mammogram, breast ultrasound, or breast biopsy might be recommended. Dr. Gorman provides comprehensive care, ensuring that every step is well-explained and patient-centric.
I’ve heard about breast self-awareness and breast self-exams. Are they necessary?
Breast self-awareness involves understanding the normal state of your breasts, while a breast self-exam helps you notice any changes. They are tools that can complement clinical breast exams and mammograms. Dr. Gorman encourages women to be proactive in their breast health.
If diagnosed with breast cancer, what are my treatment options?
Treatment options depend on the type and stage of breast cancer. They may include breast cancer surgery, hormone-blocking therapy, radiation, and chemotherapy. Dr. Gorman ensures personalized treatment, considering factors like cancer stage, genetics, and patient preference.
Is breast surgery always necessary for breast cancer treatment?
Not always. The necessity for breast cancer surgery depends on the type, stage, and location of the cancer. Dr. Gorman offers consultations to discuss the best treatment options, including breast reconstruction or prophylactic mastectomy if surgery is recommended.
How does Texas Breast Center support breast cancer survivors?
Dr. Gorman and her team at Texas Breast Center provide comprehensive cancer care, including post-surgery support and regular follow-ups. She believes in holistic care, ensuring every breast cancer survivor embarks on a healthy journey post-treatment.
How does menopause impact breast cancer risk?
Menopause, and the hormonal changes it brings, can influence breast cancer risk. Hormone replacement therapy, especially those containing progesterone, has been linked to an increased risk. Dr. Gorman advises discussing your menopause symptoms and breast cancer risk to make informed decisions.
Does breast cancer always stay in the breast?
No, breast cancer can spread or metastasize to other parts of the body, leading to metastatic breast cancer. The thorax, bones, and liver are common areas of metastasis. Early detection and understanding cancer stages are crucial, and Dr. Gorman emphasizes comprehensive screenings.
What is edema, and how is it related to breast cancer?
Edema refers to swelling caused by excess fluid. In breast cancer patients, it can be a sign of blocked lymph nodes or vessels. Monitoring for edema is a vital aspect of breast health, and Texas Breast Center offers guidance on managing and understanding this symptom.
I’ve heard of her2-negative and triple-negative breast cancers. What are they?
Both her2-negative and triple-negative refer to types of breast cancer identified by their pathology, based on the presence or absence of specific receptors. Triple-negative breast cancer lacks estrogen, progesterone, and HER2 receptors. Dr. Gorman’s expertise ensures that patients receive treatments tailored to their specific breast cancer type.
How is a fine-needle aspiration used in diagnosing breast cancer?
Fine-needle aspiration is a type of biopsy where a thin needle extracts cells from a breast mass. The samples are then studied under pathology to diagnose breast cancer or determine its type. Dr. Gorman uses this minimally invasive technique, among others, to provide accurate diagnoses.
With advancements in technology, how are radio waves used in breast cancer detection or treatment?
Radio waves are now utilized in innovative techniques like breast MRI to create detailed images. This technology can be especially beneficial in detecting tumors in women with dense breasts. At Texas Breast Center, Dr. Gorman embraces the latest in medicine and technology to ensure optimal patient care.
Is breast cancer common in the United States?
Yes, breast cancer is one of the most diagnosed cancers among women in the United States. Regular screenings and awareness are paramount. Dr. Gorman is dedicated to providing the community with the best preventative and therapeutic care.
How do medication and other treatments play a role after a breast cancer diagnosis?
Medication, including hormone therapies or targeted treatments, can be crucial in treating and preventing breast cancer recurrence. Dr. Gorman ensures that every patient receives a personalized treatment plan, considering the latest in medical research and the individual’s needs.
Breast cancer is a reality that touches many lives, and the possibility that our environment, specifically pollution, could play a role in this disease is a cause of understandable anxiety and frustration. The fear is not just about the disease itself but also about the myriad of ways it can impact your life – from personal health to family dynamics and professional responsibilities. It’s a burden that weighs heavily, not just in terms of physical health but also emotional and mental well-being.
The connection between pollution and breast cancer is a complex topic. On one hand, there are rising concerns over increasing levels of pollutants in our air, water, and soil, and on the other, a growing prevalence of breast cancer cases. This raises critical questions: Does living in a polluted environment increase the risk of breast cancer? Are there specific pollutants that are more blameworthy? How can this knowledge affect our choices and actions?
These questions are not just theoretical; they have real, tangible implications for your life and those you care about. From the anxieties of living in high-pollution areas to the decisions about preventive healthcare and lifestyle choices, the potential correlation between pollution and breast cancer affects both personal and professional aspects of life.
This article aims to delve into these concerns with clarity and depth. We will explore the various facets of pollution – its types, sources, and specific pollutants – and their established or potential links to breast cancer. With Dr. Gorman’s expertise in surgical oncology and the comprehensive approach of Texas Breast Center, we’ll guide you through the latest research, medical perspectives, and health recommendations. Our goal is to offer you information, understanding, and a path forward in addressing these critical health concerns.
As we embark on this journey of discovery and understanding, remember that you’re not alone. We’re here to share knowledge, offer support, and help navigate the complexities of breast cancer and its possible environmental triggers. Let’s uncover the truths behind pollution and breast cancer, and find ways to protect and promote our health and well-being in an ever-changing environment.
Understanding Pollution and Its Types
In our journey to unravel the complexities of pollution and its potential links to breast cancer, it is essential to start by understanding the various forms of pollution. At Texas Breast Center, Dr. Gorman emphasizes the importance of educating patients about these environmental factors, as they could play a role in breast cancer risk.
Air Pollution: Air pollution is a critical environmental concern, comprising a mix of gases and solid particles. Key components include ‘fine particulate matter’ (PM2.5 and PM10), nitrogen dioxide (NO2), sulfur dioxide, and volatile organic compounds (VOCs). These pollutants mainly originate from industrial emissions, motor vehicles, and natural sources like wildfires. Particularly, ‘fine particulate matters’, such as PM2.5 and PM10, are of significant interest due to their potential association with increased breast cancer risk. These tiny particles can penetrate deep into lung tissue and are considered highly carcinogenic.
Water Pollution: This type of pollution occurs when harmful substances contaminate water bodies. It can include heavy metals, industrial chemicals, and endocrine disruptors, originating from industrial discharge, agricultural runoff, and waste disposal.
Soil Pollution: Involves the contamination of soil with hazardous substances, including heavy metals, pesticides, and industrial chemicals. This pollution is primarily due to industrial spills, agricultural practices, and improper waste management.
Chemical Pollution: Encompasses various harmful chemicals in our environment, present in the air, water, and soil. Common sources include industrial processes, agricultural practices, and household chemicals.
Fine Particle Air Pollution and Its Links to Breast Cancer
Fine-particle air pollution, also known as fine particulate matter air pollution, is a significant environmental concern, particularly due to its potential links to breast cancer. At Texas Breast Center, Dr. Valerie Gorman emphasizes educating patients about this type of pollution, as it’s a key factor in understanding environmental health risks.
What is Fine-Particle Air Pollution?
Fine-particle air pollution consists of minuscule solids or liquids suspended in the air. These particles often include:
Dust
Dirt
Soot
Smoke
Particles in the air are categorized by size: coarse, fine, and ultrafine.
Coarse Particles (PM10): Ranging from 2.5 to 10 microns in diameter, coarse particles include substances like dust, pollen, and mold. While still a concern, these larger particles are often expelled from the body through natural mechanisms like coughing or sneezing.
Fine Particles (PM2.5): Measuring 2.5 microns or smaller in diameter, fine particles can originate from combustion processes (burning liquid fuels, coal, or wood), organic compounds (such as those in paint), or tiny pieces of metal. Due to their small size, these particles can evade the body’s natural defenses and penetrate deep into lung tissue.
Ultrafine Particles: These are even smaller, less than 0.1 microns in diameter, and are often found in cigarette smoke. Ultrafine particles can pass through lung tissue directly into the bloodstream.
Impact on Health and Breast Cancer Risk
Fine and ultrafine particles are particularly concerning for health due to their ability to bypass the body’s natural filters and deposit deep in the lungs. Once there, they can even move into other parts of the body. This trait makes them potentially more dangerous than larger particles.
The Link with Breast Cancer
Research has increasingly focused on the role of fine particulate matter (PM2.5) in breast cancer risk. These studies suggest a significant association between exposure to PM2.5 and an increased incidence of breast cancer, particularly in postmenopausal women. The mechanisms behind this link are still under investigation, but it is believed that these fine particles can induce oxidative stress, cause DNA damage, and disrupt hormonal balance, all of which are critical factors in the development of breast cancer.
At Texas Breast Center, we take these environmental factors seriously. Dr. Gorman’s approach to breast cancer treatment and care is not only focused on the medical aspects but also on understanding these broader environmental impacts. By keeping abreast of the latest research and findings in the field, we aim to provide comprehensive care that considers all potential risk factors, including those posed by fine-particle air pollution.
Breast Cancer: Types and Risk Factors
At Texas Breast Center, led by the experienced Dr. Valerie Gorman, we understand that a comprehensive knowledge of breast cancer types and their risk factors is crucial for effective diagnosis and treatment. This section aims to shed light on the various forms of breast cancer and the risk factors associated with the disease.
Types of Breast Cancer
Breast cancer, while often spoken of as a singular condition, actually encompasses several types. Each type can differ significantly in how it presents, how it affects the body, and how it should be treated.
Ductal Carcinoma In Situ (DCIS): Often considered the earliest form of breast cancer, DCIS is non-invasive. It’s confined to the milk ducts and has not spread to surrounding breast tissue.
Invasive Ductal Carcinoma (IDC): This is the most common type of breast cancer. IDC starts in the milk ducts but then breaks through the duct wall, invading the surrounding breast tissue.
Invasive Lobular Carcinoma (ILC): Starting in the lobules where breast milk is produced, ILC can spread to other parts of the breast and body.
Inflammatory Breast Cancer: A rare but aggressive type of breast cancer, this form is characterized by red, swollen, and tender breasts. It accounts for a small percentage of all breast cancer cases.
Each type of breast cancer can have different implications for treatment and prognosis, making an accurate diagnosis crucial. Dr. Gorman and her team at Texas Breast Center are skilled in diagnosing and treating all types of breast cancer, offering personalized care tailored to each patient’s unique situation.
Risk Factors for Breast Cancer
Understanding the risk factors for breast cancer is key to prevention and early detection. Some of these factors are beyond one’s control, but awareness of them can guide decisions about screening and lifestyle choices.
Age: The risk of developing breast cancer increases with age. Most breast cancers are diagnosed in women over 50 years old.
Family History and Genetics: A family history of breast cancer can increase one’s risk. Specific genetic mutations, notably BRCA1 and BRCA2, are linked to a higher risk of breast and ovarian cancers.
Hormonal Factors: Factors that increase exposure to estrogen, such as starting menstruation before age 12, going through menopause after 55, having no children or having the first child after 30, and using hormone replacement therapy (HRT), can increase breast cancer risk.
Lifestyle Factors: Lifestyle choices such as alcohol consumption, obesity, and physical inactivity can increase the risk of developing breast cancer.
Environmental Factors: Emerging research suggests that long-term exposure to certain environmental factors, like pollutants and endocrine disruptors, may play a role in increasing breast cancer risk.
At Texas Breast Center, Dr. Gorman emphasizes the importance of understanding these risk factors. She advocates for regular screenings, especially for those with higher risk, and a proactive approach to lifestyle choices to mitigate risk. By combining this knowledge with cutting-edge treatment options, we aim to provide comprehensive care that addresses both the physical and emotional aspects of breast cancer. In the next section, we will explore the current state of research on the link between pollution and breast cancer, further expanding our understanding of this complex disease.
Research Studies on Pollution and Breast Cancer
In the quest to understand the complex relationship between pollution and breast cancer, numerous research studies have been conducted. At Texas Breast Center, under the leadership of Dr. Valerie Gorman, we closely follow these studies to offer our patients the most current information and treatment options.
The research on pollution and breast cancer has brought forward several important findings and emerging trends:
Increased Breast Cancer Incidence: Studies have found a significant association between exposure to certain pollutants, especially fine particulate matter (PM2.5) and nitrogen dioxide (NO2), and an increased incidence of breast cancer. Long-term exposure to these pollutants is particularly concerning.
Postmenopausal Women at Higher Risk: Research suggests that postmenopausal women exposed to high levels of air pollution may have a higher risk of developing breast cancer. Factors like menopausal status and hormone receptor status (estrogen receptor-positive) are important in understanding this risk.
Varying Effects by Geography: Studies have shown that the risk varies by geographic location, with women in areas with higher pollution levels, such as urban areas with high traffic-related air pollution, being at greater risk.
Emerging Biomarkers: Research is also focusing on identifying biomarkers that could indicate an increased risk of breast cancer due to pollution exposure. These could be critical in early detection and prevention strategies.
Impact of Environmental Health Policies: There is growing evidence that policies aimed at reducing pollution, such as the Clean Air Act in the United States, could positively impact breast cancer incidence rates.
Dr. Gorman and the team at Texas Breast Center are committed to integrating these research insights into our patient care. We understand that staying informed about the latest findings is crucial in offering the best possible treatment and advice. Our goal is to use this knowledge to empower our patients, helping them make informed decisions about their health in a world where environmental factors are becoming increasingly important. In the following sections, we will explore the specific demographics and geographic variations in breast cancer risk and how they may be influenced by pollution.
Demographic and Geographic Variations in Breast Cancer Risk
At Texas Breast Center, led by Dr. Gorman, we recognize that breast cancer risk is not a one-size-fits-all matter. It varies significantly across different demographics and geographic regions. This section focuses on how age and geography can influence breast cancer risks and examines the variations in pollution exposure across different areas.
The Role of Age and Geography in Breast Cancer Risk
Age-Related Risk Factors: Age is a significant factor in breast cancer risk. Generally, the risk increases as women get older, with the majority of breast cancer cases diagnosed in women over 50 years old. However, younger women, particularly those in their 30s and 40s, are not immune and often face more aggressive forms of the disease.
Geographic Variations: The risk of developing breast cancer can also vary based on geographic location. For example, breast cancer incidence rates are higher in developed countries compared to developing countries. This variation could be due to differences in lifestyle factors, healthcare access, and environmental exposures.
Urban vs. Rural Areas: Women living in urban areas may face higher risks due to greater exposure to pollution. Factors like traffic-related air pollution, higher levels of nitrogen dioxide (NO2), and particulate matter can contribute to this increased risk.
Pollution Exposure and Regional Differences
Variations in Air Pollution: The level and type of air pollution can vary significantly between regions. Industrial areas and cities with heavy traffic tend to have higher concentrations of pollutants like PM2.5, NO2, and other hazardous air pollutants. These areas might see higher rates of breast cancer incidence, possibly linked to long-term exposure to these pollutants.
Impact of Environmental Policies: The effectiveness of environmental health policies, like those regulating industrial emissions and air quality, can also influence regional pollution levels. Areas with stricter pollution controls may have lower levels of air toxics, potentially reducing the risk of pollution-related breast cancers.
Historical Pollution Levels: It’s important to consider not just current but also historical pollution levels. Research has shown that long-term exposure, even to relatively low levels of certain pollutants, can impact breast cancer risk.
Global Studies: Studies from various countries, including the United States, Canada, and those in Europe, have shown differing rates of breast cancer, which could be partly attributed to variations in environmental pollution levels. For instance, the Canadian Women’s Health Study and the UK Biobank have contributed valuable data on this front.
At Texas Breast Center, understanding these demographic and geographic variations is key to providing personalized care. Dr. Gorman and her team consider these factors when advising on breast cancer screening and prevention strategies. Recognizing that pollution exposure can differ based on where a person lives, we aim to provide targeted advice and support to our patients, taking into account their unique environments and lifestyles. In our continued commitment to breast health, we ensure that every aspect of risk, from individual age to the air quality in one’s community, is considered in our comprehensive care approach.
Navigating the Path to Breast Health and Environmental Awareness
Breast cancer, as a significant health concern, has garnered attention in recent times, particularly regarding its potential links with environmental pollution. At Texas Breast Center, under the guidance of Dr. Valerie Gorman, we are deeply invested in exploring how different types of pollution might influence breast cancer risks. Our focus is especially keen on the dangers posed by fine particulate matter, a component of air pollution that includes gases and particles like PM2.5 and PM10. These particles, emerging from various sources such as industrial activities, vehicles, and natural events, have the alarming capability to penetrate lung tissue and potentially cause carcinogenic effects. Their size range, from coarse to ultrafine, renders them particularly insidious, with the smallest capable of entering directly into the bloodstream.
An integral part of our approach involves a thorough understanding of the various types of breast cancer and their associated risk factors. Breast cancer manifests in several forms, from the non-invasive Ductal Carcinoma In Situ (DCIS) to more aggressive varieties like Inflammatory Breast Cancer, each demanding a tailored approach to treatment. Risk factors for these cancers are varied, encompassing genetics, age, lifestyle choices, and possibly, exposure to environmental pollutants.
Recent research has increasingly pointed to a significant link between pollution and breast cancer, particularly noting heightened risks for postmenopausal women residing in high-pollution areas. At Texas Breast Center, we actively incorporate these research insights into our breast cancer care strategies. A key focus of ours is on early detection and crafting personalized treatment plans for our patients, taking into account their unique circumstances and needs.
Dr. Gorman, is dedicated to tackling breast cancer from all angles, including the consideration of environmental factors like pollution. We advocate for heightened awareness and proactive measures in breast health and stand ready to provide support and guidance to those seeking information or treatment. Our commitment is to offer personalized care, navigating the intricate interplay between breast cancer and environmental health, with the ultimate goal of fostering a healthier future for our patients. If you are seeking more information, guidance, or specialized care in breast health, we encourage you to reach out to Texas Breast Center. Let us join hands in navigating this journey towards better health and a brighter future.
More FAQ’s About Pollution and Breast Cancer
What is the link between pollution and breast cancer?
Recent epidemiology studies, including cohort and case-control studies, have indicated a potential link between pollution and an increased risk of breast cancer, or neoplasm of the breast. Research by institutions like the National Cancer Institute and the National Institutes of Health has focused on how pollutants like polycyclic aromatic hydrocarbons and nitrogen oxide (NOx) may affect breast tissue. Dr. Gorman at Texas Breast Center emphasizes the importance of understanding these studies for better patient education and care.
How do particulates in pollution impact breast cancer risk?
Particulates, especially those measuring 0.5 micrometres (µm) to 2.5 µm, can be inhaled and enter the circulatory system, potentially impacting the endocrine system and contributing to cancer development. The Texas Breast Center uses this information to guide mammography screenings and patient consultations, particularly for those in high pollution areas.
Does air pollution increase the mortality rate from breast cancer?
Studies, including regression analysis and meta-analysis, have suggested a correlation between exposure to air pollution and increased mortality rates from breast cancer. These studies, sometimes spanning different population groups and regions like Spain and the United States, provide vital data for healthcare providers like Dr. Gorman to assess risk factors more accurately.
What are the key variables in studying the relationship between air pollution and breast cancer?
In studies examining air pollution’s impact on breast cancer, key dependent variables often include breast cancer incidence and mortality rate, while independent variables can be various pollutants. The Texas Breast Center takes these variables into account when advising on risk factors and prevention strategies.
How do confounding factors affect the study of pollution and breast cancer?
Confounding factors, such as smoking, dietary habits, and genetic predispositions, can complicate the interpretation of studies on pollution and breast cancer. Dr. Gorman and her team at Texas Breast Center consider these factors in their comprehensive care approach, ensuring a more accurate understanding of each patient’s risk profile.
What is the role of the National Institute of Environmental Health Sciences in cancer research?
The National Institute of Environmental Health Sciences conducts research to understand the environmental factors, including air and water pollutants, contributing to diseases like cancer. This research is crucial for healthcare centers like Texas Breast Center to stay updated on the latest findings and recommendations.
How do statistical significance and confidence intervals aid in understanding breast cancer research?
Statistical significance and confidence intervals in breast cancer research help determine the reliability and precision of study findings. At Texas Breast Center, Dr. Gorman uses this statistical data to inform treatment plans and to educate patients about their breast cancer risk.
Can exposure assessment help in understanding individual risks for breast cancer?
Yes, exposure assessment, which evaluates the type and length of exposure to pollutants, is vital in understanding individual risks for breast cancer. Dr. Gorman and her team utilize exposure assessments to tailor screening and prevention strategies for their patients.
How do different particle sizes in air pollution affect breast cancer risk?
Particle sizes in air pollution, particularly those measuring 0.2 micrometres (µm), 0.5 µm, and 0.7 µm, are a focus of research due to their varying abilities to penetrate lung tissue and potentially affect breast tissue. Dr. Gorman at Texas Breast Center considers these findings crucial in understanding the etiology of breast cancer related to air pollution.
What role does ethnicity play in breast cancer studies related to pollution?
Recent cohort and case-control studies have begun to explore how breast cancer risk due to pollution varies among different ethnic groups, including Non-Hispanic whites. This research is important in the field of medicine as it helps tailor preventative strategies and treatments. Dr. Gorman utilizes these statistics to ensure personalized care for all patients at Texas Breast Center.
How does the latency period of breast cancer relate to pollution exposure?
The latency period, or the time between initial exposure to pollution and the onset of breast cancer, is a critical factor in understanding the disease’s development. The World Health Organization and the United States Environmental Protection Agency provide guidelines on these latency periods, which are considered by healthcare providers like Dr. Gorman in patient risk assessments.
What impact does smoking have on breast cancer, especially in polluted areas?
Tobacco smoking, in conjunction with exposure to air pollution, can increase the risk of diseases like lung cancer and potentially breast cancer. This mixture of pollutants complicates the epidemiology of cancer, making it a significant concern in patient education and preventive care at Texas Breast Center.
How do prospective cohort studies contribute to our understanding of breast cancer and pollution?
Prospective cohort studies follow groups of individuals over time to observe the development of breast cancer in relation to pollution exposure. These studies help identify dependent and independent variables impacting breast cancer risk and are instrumental in guiding public health policies and medical practices at institutions like Texas Breast Center.
How do census data and average pollution levels inform breast cancer research?
Census data, combined with information on average pollution density and levels in specific areas, is used to analyze the environmental impact on breast cancer incidence in various populations. This data is vital for organizations like the World Health Organization and the United States Environmental Protection Agency to create guidelines and for medical centers like Texas Breast Center to provide informed care.
How does a case–control study and prospective cohort study differ in breast cancer research related to pollution?
In breast cancer research, case-control studies compare individuals who have breast cancer to those who do not, assessing their respective exposures to pollution. On the other hand, prospective cohort studies follow a group of individuals over time to observe how their exposure to pollution might influence the development of breast cancer. Both types of studies are essential for understanding the complex relationship between pollution and breast cancer. At Texas Breast Center, Dr. Gorman utilizes findings from these studies to inform patients about their risk levels and to observe any drop in breast cancer incidence following improvements in air quality or changes in lifestyle.
Breast cancer, a complex and deeply personal journey, impacts countless lives each year. In the midst of this challenge, finding the right care and expertise is paramount. This is where Texas Breast Center, under the leadership of Dr. Valerie J. Gorman, emerges as a beacon of hope and excellence. Dr. Gorman, a renowned breast surgeon certified by the American Board of Surgery, embodies a unique blend of skill, compassion, and dedication. As Chief of Surgery and Medical Director of Surgical Services at Baylor Scott & White Medical Center – Waxahachie, her approach is not just about treating a disease but about caring for the person behind it.
The ethos of Texas Breast Center is grounded in offering an advanced, personalized, and targeted approach to breast surgery and cancer treatment. For you, the patient, this means receiving care that’s tailored to your specific needs and circumstances, ensuring the most effective treatment journey. Dr. Gorman’s expertise in surgical oncology, coupled with her commitment to patient-centric care, ensures that each patient’s experience is rooted in empathy, understanding, and the highest standard of medical excellence. This introduction to Texas Breast Center and Dr. Gorman’s work aims to guide and inform you, offering insights into how their approach can significantly benefit your journey through breast cancer treatment.
Questions to Ask a Dallas Breast Cancer Surgeon
When seeking the best breast cancer surgeon in Dallas, it’s important to ask the right questions to ensure you receive the highest quality of care. Here are some key questions to consider, answered by Dr. Valerie J. Gorman and the Texas Breast Center:
What are your qualifications and experience in breast cancer surgery?
Generally, a qualified breast cancer surgeon should be board-certified and have extensive experience in surgical oncology, specifically in breast surgeries. Dr. Gorman is board-certified by the American Board of Surgery and has a focused specialization in surgical oncology and surgical diseases of the breast. Her experience as Chief of Surgery and Medical Director of Surgical Services at Baylor Scott & White Medical Center – Waxahachie further validates her expertise.
How do you approach treatment planning for breast cancer patients?
A top surgeon should emphasize a personalized treatment plan, considering the patient’s medical history, type of breast cancer, and individual needs. At Texas Breast Center, Dr. Gorman prioritizes a tailored approach. She evaluates each patient’s unique situation to develop a targeted treatment plan, ensuring it aligns with both medical and personal needs.
What types of breast cancer surgeries do you perform?
It’s crucial that your surgeon is skilled in various breast cancer surgeries. Dr. Gorman is proficient in a wide range of procedures, from lumpectomies to mastectomies, ensuring that each surgery is suited to the specific type of breast cancer and patient preference.
Can you describe your post-operative care and follow-up process?
Post-operative care is as important as the surgery itself. At Texas Breast Center, Dr. Gorman and her team provide comprehensive post-operative care, including regular follow-ups, to monitor recovery and address any concerns promptly.
How do you incorporate new technologies or treatments into your practice?
Staying abreast of the latest medical advancements is vital. Dr. Gorman integrates the latest technologies and treatment modalities into her practice at Texas Breast Center, ensuring her patients receive the most advanced care available.
What support services are available for patients?
Holistic care often includes support services like counseling or therapy. Texas Breast Center, under Dr. Gorman’s guidance, offers various support services, acknowledging the emotional and psychological aspects of dealing with breast cancer.
By asking these questions, you can gain a comprehensive understanding of a surgeon’s expertise and approach to care, helping you make an informed decision. Dr. Gorman’s responses highlight the commitment of Texas Breast Center to provide exceptional, personalized care for each patient.
Why did Texas Breast Center choose to be close to Dallas?
Texas Breast Center’s decision to be situated near Dallas is a strategic one, influenced by a combination of factors that align with their mission to provide exceptional breast cancer care.
Access to a Larger Population: Dallas is one of the largest cities in Texas, offering a vast and diverse population base. Being close to such a metropolitan area allows Texas Breast Center to serve a larger community, extending its reach to more patients who can benefit from their specialized breast cancer care.
Healthcare Infrastructure: Dallas is known for its robust healthcare infrastructure, including advanced medical facilities, research institutions, and a network of healthcare professionals. This environment fosters collaboration, innovation, and access to the latest medical advancements, which are crucial for a specialty center like Texas Breast Center.
Patient Convenience: For patients undergoing treatment, proximity to a major city like Dallas means easier access to comprehensive care. It reduces travel time and stress, especially important for those requiring frequent visits or long-term treatment plans.
Professional Opportunities: Being near a major urban center like Dallas attracts top medical professionals and allows for continuous professional development. This ensures that Texas Breast Center can maintain a team of highly skilled and up-to-date professionals, like Dr. Gorman, who are well-versed in the latest techniques and treatments in breast cancer care.
Community Engagement and Awareness: Being close to Dallas also allows Texas Breast Center to engage more effectively with the community in terms of education and awareness programs about breast cancer. This is essential for early detection and prevention strategies, which are key components of effective breast cancer management.
Overall, Texas Breast Center’s location near Dallas is a thoughtful choice that reflects our commitment to providing accessible, advanced, and patient-centric breast cancer care, leveraging the advantages offered by a major metropolitan area.
Dallas Breast Cancer Surgery
Breast cancer surgery is a critical component of breast cancer treatment, and its approach can vary significantly depending on the individual case. At Texas Breast Center, led by Dr. Valerie J. Gorman, the approach to breast cancer surgery is centered around the patient’s unique needs and the specifics of their diagnosis.
Dr. Gorman, a board-certified breast surgeon, specializes in a range of surgical procedures that target breast cancer. Her expertise encompasses both lumpectomies, which involve the removal of the tumor and some surrounding tissue, and mastectomies, where the entire breast is removed. The choice between these procedures depends on various factors such as the size and location of the tumor, the stage of the cancer, and the patient’s personal preferences and overall health.
What sets Dr. Gorman and Texas Breast Center apart is their commitment to a personalized approach. Each patient’s surgery plan is carefully crafted, taking into consideration not only the medical aspects of their cancer but also their emotional and psychological well-being. Dr. Gorman believes in empowering her patients with information and involving them in the decision-making process, ensuring that they are comfortable and confident in their treatment plan.
Furthermore, the use of advanced surgical techniques and technology is a hallmark of Dr. Gorman’s practice. She stays abreast of the latest developments in surgical oncology to provide her patients with the most effective, minimally invasive options available. This not only improves the surgical outcomes but also aids in quicker recovery and better cosmetic results.
Post-surgery, the care at Texas Breast Center continues with a thorough follow-up regimen. Dr. Gorman and her team closely monitor the patient’s recovery, addressing any complications and providing support throughout the healing process. The goal is to ensure that each patient not only survives but thrives after breast cancer surgery, with the best possible quality of life.
In summary, breast cancer surgery at Texas Breast Center under Dr. Gorman’s guidance is more than a medical procedure. It is a comprehensive, compassionate journey tailored to each patient, combining surgical excellence with a deep understanding of the personal challenges faced by those battling breast cancer.
Why We Love Dallas, TX
At Texas Breast Center, our affinity for Dallas, TX, is deeply rooted in the city’s unique character and dynamic growth. As the largest city in Dallas County and a key part of the Dallas–Fort Worth metroplex, Dallas stands out not only for its significant population and cultural diversity but also for its rich history and economic vibrancy.
Dallas, with a population exceeding 1.3 million, is a melting pot of cultures, ideas, and innovations. It’s the hub of a metropolitan area that is unparalleled in the Southern United States, both in terms of size and the absence of a navigable link to the sea. The city’s growth was initially spurred by the development of major railroad lines and later bolstered by the advent of the Interstate Highway System. These developments transformed Dallas into a crucial industrial, financial, and transportation center.
The city’s diverse economy is powered by sectors like defense, financial services, information technology, telecommunications, and transportation. Home to nine Fortune 500 companies, including prominent names like American Airlines Group, AT&T, and Texas Instruments, Dallas is a beacon of economic opportunity. Baylor Scott & White, our parent organization, is part of this thriving economic landscape. As the largest not-for-profit healthcare system in Texas, Baylor Scott & White’s presence in Dallas exemplifies the city’s role as a healthcare leader.
Education and diversity are at the heart of Dallas’ identity. The metropolitan area boasts over 41 colleges and universities, a testament to its commitment to education and innovation. The city is celebrated for its rich tapestry of racial, cultural, and religious backgrounds, hosting one of the largest LGBT communities in the U.S. In 2018, it was ranked as the fifth most diverse city in the nation by WalletHub.
Culturally, Dallas is a treasure trove. From the African American Museum to the Latino Cultural Center, and from the Dallas Museum of Fine Arts to the iconic State Fair of Texas held at Fair Park, the city’s cultural offerings are as diverse as its population. These cultural institutions not only enrich the lives of residents but also attract visitors from across the globe, adding to the city’s vibrant social fabric.
Being part of the Dallas-Fort Worth community is a source of pride for Texas Breast Center. The city’s dynamic blend of history, diversity, economic strength, and cultural richness makes it an ideal location for providing advanced and empathetic healthcare, just as we strive to do every day.
DRIVING DIRECTIONS FROM DOWNTOWN DALLAS
More FAQ’s About Dallas Breast Cancer Surgeon
What is the difference between a lumpectomy and a mastectomy, and how does Dr. Gorman decide which is best?
A lumpectomy involves removing the breast tumor and a small margin of surrounding tissue, while a mastectomy involves removing the entire breast. Dr. Gorman, a distinguished Doctor of Medicine, evaluates factors like the size and location of the tumor, the stage of malignancy, and the patient’s preferences. At Texas Breast Center, both procedures are performed with precision and care, aligned with the standards of the American Society of Breast Surgeons and the American College of Surgeons.
How does Texas Breast Center use imaging techniques like mammography, magnetic resonance imaging, and medical ultrasound in breast cancer diagnosis?
Imaging techniques are crucial in the medical diagnosis of breast cancer. Mammography is typically the first step, followed by more detailed imaging like magnetic resonance imaging (MRI) or medical ultrasound if a breast mass or abnormality is detected. At Texas Breast Center, Dr. Gorman utilizes these techniques to accurately identify and assess breast cancer, ensuring a comprehensive evaluation for each patient.
Can you explain the role of a biopsy in diagnosing breast cancer, and what types does Dr. Gorman perform?
A biopsy is essential for confirming a breast cancer diagnosis. Types include fine-needle aspiration, which uses a thin needle to extract tissue or fluid, and a core biopsy, where a larger needle is used. Dr. Gorman at Texas Breast Center also performs lymph node biopsies, including sentinel lymph node biopsies, to check for cancer spread. This aligns with her fellowship training in breast surgical oncology and her commitment to precise, minimally invasive diagnostic methods.
What is the importance of lymph node dissection and lymphadenectomy in breast cancer surgery?
Lymph node dissection and lymphadenectomy involve removing lymph nodes to check for cancer spread, which is vital for staging and treatment planning. Dr. Gorman, an expert in general surgery and breast cancer surgery, performs these procedures when necessary, with a focus on minimizing risk and maximizing outcomes. Her approach is informed by her residency at the University of Texas Southwestern Medical Center and her membership in the Society of Surgical Oncology.
What should I know about radiation therapy as a part of breast cancer treatment at Texas Breast Center?
Radiation therapy is often used after breast-conserving surgery like a lumpectomy to eliminate any remaining cancer cells. At Texas Breast Center, Dr. Gorman collaborates with radiation oncologists to tailor this treatment to each patient’s needs. She considers factors like the tumor’s location and the patient’s overall health to optimize outcomes, drawing on her extensive medical school training and experience in breast surgery.
How does Dr. Gorman address breast pain or nipple discharge in patients at Texas Breast Center?
Breast pain and nipple discharge can be symptoms of various breast conditions, not always cancer. Dr. Gorman evaluates these symptoms through a comprehensive assessment, including a physical examination and diagnostic imaging. Her approach reflects the best practices of the Association of Women Surgeons and preventive healthcare principles, ensuring that each patient receives accurate diagnosis and appropriate care.
Is preventive mastectomy an option at Texas Breast Center, and what are the considerations?
Preventive mastectomy is considered for individuals at high risk of developing breast cancer. Dr. Gorman assesses this risk based on factors like family history and genetic predisposition. As a surgeon affiliated with a top-tier hospital in North Texas, she ensures that her patients are fully informed about this option, supporting them through the decision-making process with empathy and expertise.
How do cancer centers like Texas Breast Center approach the treatment of breast cancer, and what role do breast specialists play?
Cancer centers, including Texas Breast Center, approach the treatment of breast cancer with a comprehensive strategy. Breast specialists like Dr. Gorman collaborate with a team of experts in medical oncology, radiation therapy, and reconstructive or plastic surgery to offer personalized treatment plans. This team approach ensures each aspect of breast cancer, from diagnosis to surgical management, is handled with utmost care and expertise.
Can you explain the importance of breast cancer staging and how it guides treatment decisions at Texas Breast Center?
Breast cancer staging is crucial in determining the extent of the cancer and the most effective treatment strategy. At Texas Breast Center, staging is conducted through advanced breast imaging techniques, including breast MRI, and breast biopsy. Dr. Gorman, along with her team, uses this information to plan targeted therapy, surgery, and other treatments, ensuring each patient receives the most appropriate care for their specific stage of cancer.
What options are available for reconstructive surgery and oncoplastic surgery at Texas Breast Center?
Reconstructive surgery and oncoplastic surgery are vital components of breast cancer treatment for many patients. At Texas Breast Center, Dr. Gorman offers a range of options for breast reconstruction, combining oncology research insights and surgical expertise to achieve the best aesthetic and functional outcomes. Her approach to oncoplastic surgery focuses on removing cancer while preserving or restoring the breast’s appearance.
How does genetic testing and genetic risk evaluation factor into breast cancer treatment at Texas Breast Center?
Genetic testing and risk evaluation are integral in assessing a patient’s susceptibility to breast cancer. Texas Breast Center, under Dr. Gorman’s guidance, utilizes genetic testing to identify patients with a higher genetic risk for breast cancer. This information is crucial in tailoring preventive strategies and treatment plans, including decisions about preventive mastectomy and targeted therapy.
In terms of education and training, how does Dr. Gorman’s background and residency programs contribute to her expertise as a breast cancer surgeon?
Dr. Gorman’s educational background, including her residency programs and training at prestigious institutions like UT Southwestern Medical Center, has equipped her with deep knowledge and skills in the surgical management of breast cancer. Her extensive training in general surgery and breast surgery, combined with ongoing participation in breast cancer research and oncology research, ensures that she remains at the forefront of advancements in breast cancer care.
What is the approach to benign breast conditions and cancer awareness at Texas Breast Center?
At Texas Breast Center, benign breast conditions are treated with the same level of care and attention as cancerous conditions. Dr. Gorman and her team provide thorough evaluations and treatment options for breast lumps and other non-cancerous breast issues. Additionally, the center actively participates in cancer awareness initiatives, educating the community about breast health, early detection, and the importance of regular breast imaging and breast exams.
When faced with a breast cancer diagnosis, patients have many questions that immediately come to mind. Dr. Gorman is often asked how soon surgery needs to be performed after a breast cancer diagnosis. While each situation is unique, this article will give a basic explanation of the general guidelines for when surgery should be performed after a breast cancer diagnosis. At Texas Breast Center, our goal is to help patients find the most minimally invasive treatment with the best outcome for their particular type of breast cancer. Dr. Gorman is dedicated to offering her patients the most advanced, personalized, and targeted approach to treating breast cancer with breast surgery.
How soon will I need surgery after breast cancer diagnosis?
After being diagnosed with breast cancer it’s best to have surgery between 31 to 90 days after being diagnosed. This gives enough time for all the necessary tests and for patients to make informed decisions about their treatment without impacting their chances of survival.
After finding out you have breast cancer, deciding when to have surgery is a very important first step you’ll make with Dr. Gorman. At Texas Breast Center, Dr. Gorman and her team work closely with patients to determine the best time for your breast cancer surgery.
Upon receiving a medical diagnosis of breast cancer, the pathway to treatment often begins with an assessment of the neoplasm by a physician specializing in oncology, focusing on the intricate relationship between the tumor’s receptor status, such as HER2 and hormone receptor presence, and the disease’s overall pathology. This is vital for tailoring the treatment of cancer to each woman’s unique case.
Surgery is often the first step in treating breast cancer. In some cases, the doctor might suggest starting with chemotherapy first to shrink the cancer before surgery.
The decision-making process is supported by comprehensive diagnostic tools, including mammography and magnetic resonance imaging (MRI), to accurately stage the cancer and evaluate its spread to the lymphatic system, ensuring a targeted surgical approach. The integration of neoadjuvant therapy, which may include radiation therapy or systemic treatments based on the tumor’s biology, such as epidermal growth factor receptor (EGFR) inhibitors for HER2-positive or triple-negative breast cancer, is also considered to optimize outcomes.
There are three main types of surgery for breast cancer: lumpectomy, mastectomy, and lymph node removal. A lumpectomy removes just the part of the breast with cancer, trying to save as much of the breast as possible. A mastectomy removes the whole breast, and sometimes women choose to have both breasts removed as a way to prevent cancer from spreading or coming back.
In the realm of surgical oncology, the choice between breast-conserving surgery and mastectomy, including variations like skin-sparing or simple mastectomy, is informed by a multitude of factors, including tumor size, location, and the patient’s health care preferences, often discussed in detail with the surgeon. The role of genetic testing and biomarkers in guiding these decisions underscores the importance of a personalized treatment plan, incorporating adjuvant therapy as necessary to address microscopic disease or metastasis, thereby enhancing the survival rate.
However, there are valid reasons for sometimes delaying treatment slightly, whether for further consultations, arranging personal affairs, or psychological preparedness. Yet, it’s important to be aware of the risks associated with delaying treatment too long. A study published on March 1, 2023, in JAMA Surgery, found that women who waited longer than eight weeks to have surgery after an early breast cancer diagnosis did not do as well.
In short, choosing when to have surgery after a breast cancer diagnosis involves finding the right balance between acting quickly and taking enough time to be sure about your treatment plan. Dr. Gorman and her team at Texas Breast Center are dedicated to helping patients through this process, offering support and expertise to ensure the best outcome.
How long is too long to wait to have surgery after breast cancer diagnosis?
When navigating the journey from breast cancer diagnosis to surgery, a common concern among patients at Texas Breast Center, under Dr. Gorman’s care, is the length of time they should wait before undergoing surgery. Understanding that the timing of surgery can significantly impact a patient’s prognosis, the goal is to find a balance between acting promptly and allowing sufficient time for necessary preoperative evaluations and thoughtful decision-making.
The medical community’s research on the ideal timing for breast cancer surgery presents varied findings. Some studies, including those conducted in 2017 and 2022, suggest that the prognosis for breast cancer patients does not begin to decline until the time to surgery exceeds 60 days. This insight provides patients and their healthcare teams with a broad window to complete all necessary preparations without rushing the process unduly.
Further examination of this topic was provided by a 2018 review, which analyzed multiple studies to assess how the timing of treatment impacts patient outcomes. The author of this review highlighted that undergoing surgery within 90 days of diagnosis appears to be the best approach to ensure a favorable prognosis. This recommendation aligns with the findings of a 2020 study, which emphasized the benefits of scheduling the first treatment between 31 to 90 days post-diagnosis. This timeframe not only facilitates comprehensive diagnostic testing and deliberate decision-making but also maintains the integrity of the patient’s survival chances.
For patients and the medical team at Texas Breast Center, these insights underline the importance of a measured approach to planning surgery after a breast cancer diagnosis. While it is crucial to proceed without unnecessary delay, allowing for a period that supports thorough testing and informed consent can be equally critical to achieving the best possible outcomes. Dr. Gorman and her team are dedicated to guiding their patients through this process, ensuring that each step is taken with precision and care to optimize the outlook for every individual they treat.
Texas Breast Center’s Target Approach to Treatment
The approach to breast cancer treatment at Texas Breast Center, led by Dr. Gorman, is rooted in personalized care, cutting-edge treatment, and a commitment to finding the most minimally invasive options for our patients. We understand the urgency and the complexities involved in making such a critical decision following a breast cancer diagnosis. Our aim is to ensure that every patient feels supported, informed, and confident in their treatment plan. If you or a loved one is navigating this challenging journey, we encourage you to reach out to us. Let’s work together to determine the best course of action for your specific situation, keeping in mind the importance of timely intervention while also allowing for thorough preparation and peace of mind. Dr. Gorman and her dedicated team are here to offer the expertise and compassionate care you deserve, every step of the way.
More FAQ’s About How Soon Will I Need Surgery After Breast Cancer Diagnosis
What is the typical waiting period for surgery after a breast cancer diagnosis at Texas Breast Center?
At Texas Breast Center, the typical waiting period for surgery after a breast cancer diagnosis ranges between 31 to 90 days. This timeframe allows Dr. Gorman and her team to conduct thorough diagnostic testing and for patients to make informed decisions about their treatment plan without compromising their prognosis.
Can the timing of surgery impact my prognosis?
Yes, the timing of surgery can impact your prognosis. At Texas Breast Center, we strive to schedule surgery within an optimal window that allows for comprehensive evaluation and preparation, while also addressing the cancer in a timely manner to ensure the best possible outcomes for our patients.
How does Dr. Gorman determine the urgency of surgery for breast cancer patients?
Dr. Gorman evaluates the urgency of surgery for breast cancer patients based on several factors, including the type and stage of cancer, the patient’s overall health, and the results of diagnostic tests. This personalized approach ensures that each patient at Texas Breast Center receives care tailored to their specific needs.
Is it possible to delay surgery for breast cancer?
While surgery is typically recommended within a specific timeframe, there are circumstances under which a slight delay might be considered at Texas Breast Center. These can include the need for additional diagnostic tests, the patient’s psychological readiness, or personal reasons. However, Dr. Gorman carefully weighs the potential risks of any delay against the benefits.
What happens if surgery is delayed beyond the recommended timeframe?
Delaying surgery beyond the recommended timeframe can impact the effectiveness of treatment and potentially affect prognosis. At Texas Breast Center, Dr. Gorman and her team work diligently to prevent unnecessary delays and to communicate the importance of timely surgery to our patients, ensuring they understand the risks involved.
How soon after chemotherapy can I have surgery?
If chemotherapy is part of your pre-surgery treatment plan, the timing of surgery after chemotherapy will depend on your response to the treatment and your overall health. Dr. Gorman at Texas Breast Center evaluates each patient’s situation to schedule surgery at the most opportune time, typically allowing for a recovery period after chemotherapy.
What preoperative tests are required before surgery?
Before surgery, patients at Texas Breast Center may undergo a range of preoperative tests, including blood tests, imaging studies like mammograms or MRIs, and possibly a biopsy to evaluate the cancer’s characteristics. These tests help Dr. Gorman plan the most effective surgical approach.
How does the type of breast cancer affect surgery timing?
The type of breast cancer can significantly affect the timing of surgery. At Texas Breast Center, aggressive or rapidly growing cancers may require more immediate intervention, while slower-growing cancers might allow for a slightly longer preparation period. Dr. Gorman tailors the timing based on the cancer’s behavior and patient needs.
What role does my overall health play in surgery timing?
Your overall health is a crucial factor in determining the timing of surgery. At Texas Breast Center, Dr. Gorman assesses each patient’s health status to ensure they are physically ready for surgery and to minimize the risk of complications, adjusting the treatment timeline as necessary.
How can I prepare for surgery once my date is set?
Once your surgery date is set at Texas Breast Center, Dr. Gorman and her team will provide you with detailed instructions on how to prepare, including guidelines on eating, drinking, medication adjustments, and what to bring to the hospital. We also emphasize the importance of mental preparation and offer support resources to help our patients feel ready for the next step in their treatment journey.
How do early detection and clinical trial participation impact breast cancer management and treatment?
Early detection of breast cancer through screening methods like diagnostic mammograms and ultrasounds enables the use of less invasive treatments by identifying the disease at an early stage. Additionally, participating in clinical trials gives patients access to cutting-edge therapies, particularly beneficial for hard-to-treat subtypes like triple-negative or HER2-negative breast cancers, thus contributing to advances in breast cancer management.
How does the evaluation of axillary lymph nodes affect breast cancer treatment?
The evaluation of axillary lymph nodes through methods like fine-needle aspiration or surgical biopsy is essential for staging breast cancer and assessing the disease’s spread. This process informs the decision on systemic therapies to prevent distant recurrence and involves a team of specialists to ensure a treatment approach that maximizes tissue and skin preservation.
How does Texas Breast Center address the anxiety patients feel after a breast cancer diagnosis?
Texas Breast Center provides a supportive environment that offers detailed information and guidance on insurance, treatment options, and the emotional challenges of breast cancer, reflecting Dr. Gorman’s commitment to cancer treatment advancement through personalized, compassionate care.
Breast cancer remains one of the most commonly diagnosed cancers worldwide, making understanding its causes, particularly those related to lifestyle, incredibly important. Despite advancements in cancer research, prevention, and care, many are unaware of the significant role that lifestyle choices, such as diet, exercise, and alcohol consumption, play in the development of this disease. Dr. Gorman of Texas Breast Center is deeply committed to providing her patients with an advanced, personalized, and targeted approach to breast surgery and the treatment of breast cancer. Recognizing the importance of a comprehensive approach to cancer prevention and care, this article will delve into the many lifestyle risks associated with breast cancer.
Dr. Gorman and Texas Breast Center team understand that an essential aspect of breast health involves educating patients about the various lifestyle factors that can influence their risk of developing breast cancer. It is crucial to understand the connection between lifestyle choices and breast cancer risk to implement necessary lifestyle changes and engage in cancer-preventive behaviors. This article aims to provide a thorough examination of the relationship between lifestyle risks and breast cancer. By exploring these topics, this article hopes to empower individuals with the information needed to take proactive steps toward reducing their risk of breast cancer and promoting breast health.
Alcohol Consumption
Increased alcohol consumption is a significant lifestyle risk factor for breast cancer, with even small amounts raising estrogen levels and thereby increasing the risk. The American Cancer Society advises limiting alcohol to one drink per day, though some, especially those with a family history of breast cancer, may choose to abstain entirely. The type of alcohol consumed may also impact risk, with higher alcohol content beverages, like hard liquor, potentially posing a higher risk than beer or wine.
Dr. Gorman and her team at Texas Breast Center emphasize the importance of understanding the risks associated with alcohol consumption and breast cancer. They provide personalized recommendations for managing alcohol intake as part of a comprehensive approach to reducing breast cancer risk and optimizing overall health.
Physical Inactivity
Physical inactivity significantly increases breast cancer risk, and maintaining regular physical activity can regulate hormone levels associated with breast cancer development. Regular exercise and physical activity are vital for reducing breast cancer risk by maintaining healthy body weight and regulating hormone levels. Dr. Gorman at Texas Breast Center encourages regular exercise, aligning with the American Cancer Society’s recommendation of at least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity exercise per week as part of a comprehensive approach to breast health and cancer prevention. Starting slowly and consulting healthcare professionals like Dr. Gorman before beginning a new regimen is essential, especially for those with existing health conditions or a higher breast cancer risk. They encourage patients to enjoy physical activities regularly, benefiting not only breast cancer prevention but also overall health by reducing the risk of other cancers, heart disease, stroke, osteoporosis, managing stress, and improving mood. In summary, regular physical activity reduces breast cancer risk and has multiple health benefits, and Dr. Gorman’s team is dedicated to helping patients incorporate it into their daily routine to improve overall health and well-being.
Diet
A balanced, nutritious diet is vital for reducing breast cancer risk. High-fat diets, processed foods, and low intake of fruits and vegetables contribute to increased risk, while maintaining a healthy weight, reducing inflammation, and consuming essential nutrients can lower it. Dr. Gorman and Texas Breast Center team recommend a balanced diet with fruits, vegetables, whole grains, lean proteins, and healthy fats, limiting processed foods, sugary and alcoholic beverages, and excessive red or processed meat. Research suggests a Mediterranean diet and possibly a high soy diet, combined with regular physical activity and limited alcohol consumption, is the most effective approach, although the evidence on soy is mixed. In summary, a nutrient-dense diet can lower breast cancer risk and improve overall health. Dr. Gorman and her team are dedicated to helping patients make informed dietary choices and develop healthy eating habits for long-term breast health and overall well-being.
Obesity
Obesity, particularly after menopause, is a significant breast cancer risk factor, linked to increased estrogen production, insulin levels, and poorer prognosis for diagnosed individuals. Dr. Gorman of Texas Breast Center emphasizes the importance of healthy weight management through a balanced diet, regular physical activity, and behavioral changes, promoting a gradual weight loss of 0.5 to 1 kg per week. She provides personalized support for her patients to develop a sustainable plan, set realistic goals, and seek necessary support, as it is not only about reducing breast cancer risk but also promoting overall well-being. In summary, maintaining a healthy weight can lower breast cancer risk, and Dr. Gorman and her team are committed to supporting their patients in managing their weight and reducing their breast cancer risk.
Smoking
Long-term smoking is linked to a modest increase in breast cancer risk, especially in premenopausal women, and various other health risks, such as lung cancer, cardiovascular disease, and stroke. Dr. Gorman and Texas Breast Center team advise against smoking and provide support and resources for those wishing to quit. Although the breast cancer risk associated with smoking is modest compared to obesity or family history, quitting smoking improves overall health. Passive smoking may also increase breast cancer risk, so avoiding secondhand smoke is advised. Dr. Gorman is committed to supporting patients in their journey to quit smoking. In summary, quitting smoking is crucial for reducing breast cancer risk and promoting overall health, and Texas Breast Center team is dedicated to helping patients quit smoking and improve their well-being.
Night Shift Work
Night shift work can disrupt circadian rhythms and melatonin production, potentially increasing breast cancer risk, although evidence is not entirely consistent. Dr. Gorman at Texas Breast Center advises patients to practice good sleep hygiene, including a regular sleep schedule and minimizing screen exposure before bedtime, and for those working night shifts, wearing blue light-blocking glasses and maintaining a regular sleep schedule on days off. While the increase in risk is modest compared to other factors like obesity or family history, it is a modifiable risk factor worth considering. In summary, practicing good sleep hygiene and minimizing artificial light exposure at night can help reduce breast cancer risk. Dr. Gorman and her team provide personalized recommendations and support to manage breast cancer risk and promote overall well-being.
Maintaining a Healthy Weight
Maintaining a healthy weight is vital for reducing breast cancer risk, particularly postmenopausal women, as obesity increases estrogen and insulin levels, both linked to higher breast cancer risk. Dr. Gorman and her team at Texas Breast Center offer personalized support for lifestyle changes like a healthy diet and regular physical activity. While BMI is a common measure of healthy weight, it doesn’t consider muscle mass, bone density, or body composition. Overall, a healthy weight reduces breast cancer risk and benefits overall health. Dr. Gorman’s team provides personalized recommendations to help patients maintain a healthy weight and improve their well-being.
Take Control of Your Health Today!
Breast cancer risk is influenced by several factors, including obesity, night shift work, smoking, physical inactivity, poor diet, and unhealthy body weight. Dr. Gorman and her team at Texas Breast Center are dedicated to helping patients manage these modifiable risk factors through personalized recommendations and support. Achieving a healthy weight, engaging in regular physical activity, consuming a balanced diet, avoiding smoking and excessive alcohol consumption, and managing exposure to artificial light at night can all contribute to reducing breast cancer risk and promoting overall health and well-being.
Take control of your health today by making positive lifestyle changes that can reduce your risk of breast cancer and improve your overall well-being. Schedule an appointment with Dr. Gorman and her team at Texas Breast Center to receive personalized recommendations and support tailored to your unique needs and circumstances. Remember, a healthier you is possible, and it starts with taking the first step towards a brighter, healthier future. Act now to take control of your health and reduce your breast cancer risk!
Frequently Asked Questions About Breast Cancer Causes: Lifestyle Risks
What types of breast cancer are most common, and how does weight gain affect my risk?
There are several types of breast cancer, but the most common ones are ductal carcinoma in situ (DCIS), invasive ductal carcinoma, and invasive lobular carcinoma. Weight gain, especially after menopause, increases the risk of breast cancer due to higher estrogen production in fat tissue. Maintaining a healthy body weight is crucial for reducing the risk of breast cancer and other health issues. At Texas Breast Center, we provide personalized support and recommendations to help our patients maintain a healthy weight and reduce their breast cancer risk.
How does hormone therapy and hormone replacement therapy affect breast cancer risk?
Hormone therapy, specifically menopausal hormone therapy (MHT) and hormone replacement therapy (HRT), is associated with an increased risk of breast cancer. Combined oral contraceptive pills, which contain estrogen and progestin, also slightly increase the risk of breast cancer. However, the risk decreases over time once these medications are stopped. It’s important to discuss the risks and benefits of hormone therapy with your healthcare provider. At Texas Breast Center, we provide personalized recommendations to help our patients make informed decisions about their health.
Does drinking alcohol or smoking increase my risk for breast cancer?
Yes, drinking alcohol and smoking are both associated with an increased risk of breast cancer. The risk increases with the amount of alcohol consumed and the duration of smoking. It is advisable to limit alcohol consumption to moderate levels or avoid it altogether and to quit smoking. At Texas Breast Center, we provide resources and support for those who wish to quit smoking and limit alcohol consumption.
Is there a link between breast density and breast cancer?
Yes, having dense breast tissue is a known risk factor for breast cancer. Dense breast tissue can make it harder for mammograms to detect breast cancer, and women with dense breasts may need additional screening tests. It is important to discuss your breast density and what it means for your screening guidelines with your healthcare provider. At Texas Breast Center, we provide personalized screening recommendations based on each patient’s unique needs and circumstances.
What are the signs and symptoms of breast cancer?
Common signs and symptoms of breast cancer include a lump in the breast or underarm, changes in the size, shape, or appearance of the breast, unexplained pain in the breast or nipple, nipple discharge, and skin changes on the breast. However, it is important to note that many breast conditions that cause similar symptoms are not cancerous. Early detection is crucial for successful treatment, so it is important to have regular breast cancer screenings and to consult a healthcare professional if you notice any unusual changes in your breasts. At Texas Breast Center, we are committed to providing comprehensive breast health care, including screening, diagnosis, and treatment.
What is the role of genetics and BRCA mutation in breast cancer?
Genetics play a significant role in breast cancer risk. Specific genetic mutations, such as BRCA1 and BRCA2, significantly increase the risk of developing breast and ovarian cancer. It is important to discuss your family history of cancer and consider genetic testing if you have a strong family history of breast or ovarian cancer. At Texas Breast Center, we provide genetic counseling and testing to help our patients understand their risk and make informed decisions about their health.
Can physical activity and diet reduce the risk of breast cancer?
Yes, regular physical activity and a healthy diet can reduce the risk of breast cancer. The American Cancer Society recommends at least 150 minutes of moderate-intensity exercise or 75 minutes of vigorous-intensity exercise per week for cancer prevention. A diet rich in fruits, vegetables, whole grains, lean protein, and healthy fats can also contribute to lower breast cancer risk and improve overall health. At Texas Breast Center, we provide personalized recommendations and support to help our patients incorporate regular physical activity and a healthy diet into their daily routine.
Is breast cancer screening necessary for all women?
Breast cancer screening is important for all women, but the screening guidelines may vary based on individual risk factors such as age, family history, and breast density. Regular mammograms are recommended for women starting at age 40 or 50, depending on individual risk factors. It is important to discuss your personal risk factors and screening recommendations with your healthcare provider. Texas Breast Center provides personalized screening recommendations based on each patient’s unique needs and circumstances.
What are the options for breast reconstruction surgery after mastectomy?
Breast reconstruction surgery can be done using several different methods, including implants, tissue flaps, or a combination of both. The best method for you will depend on your individual circumstances, including your overall health, the size and shape of your breasts, and your personal preferences. It is important to discuss your options and the potential risks and benefits of each method with your healthcare provider. At Texas Breast Center, we provide personalized recommendations and support to help our patients make informed decisions about their breast reconstruction options.
How does being overweight or obese impact my risk of developing breast cancer?
Being overweight or obese is associated with increased levels of estrogen and insulin in the body, which can elevate the risk of breast and endometrial cancer. Excess fatty tissue increases estrogen production, which is a known risk factor for breast cancer, especially in postmenopausal women. The Texas Breast Center can help with personalized recommendations for maintaining a healthy weight and reducing cancer risk.
Can oral contraceptives or hormone replacement therapy increase my risk of breast cancer?
Yes, using oral contraceptives or postmenopausal hormone therapy, especially those containing both estrogen and progestin, can slightly increase the risk of developing breast cancer. Bioidentical hormone therapy and contemporary hormonal contraception have similar risks. It’s essential to discuss your personal history and risk factors with your healthcare provider at the Texas Breast Center before starting any hormone therapy or birth control medicine.
How does smoking and alcohol consumption affect my breast cancer risk?
Exposure to cigarette smoke and drinking alcohol increases the risk of developing breast cancer. Alcohol raises estrogen levels in the body, while toxins in cigarette smoke can damage DNA in breast cells, leading to invasive cancer. The Texas Breast Center recommends smoking cessation, limiting alcohol intake, and adopting a healthy lifestyle to reduce your risk.
Does my diet play a role in breast cancer prevention?
Absolutely. A balanced diet rich in fruits, vegetables, whole grains, lean proteins, and low in processed foods, sugary beverages, and red meat can contribute to breast cancer prevention. Some studies suggest that a plant-based whole food diet, high in soy products, and low in western dietary pattern foods can reduce breast cancer risk. However, the evidence on soy products is mixed, and more research is needed. The Texas Breast Center provides personalized dietary recommendations and support to help you maintain a healthy diet and reduce your breast cancer risk.
How can I modify my breast cancer risk, and does pregnancy or breastfeeding affect my risk?
Being physically active, maintaining a healthy weight, and practicing mindfulness-based stress reduction can help modify breast cancer risk. Pregnancy and breastfeeding can lower your risk, as can limiting exposure to estrogen therapy and hormone replacement therapy. Having a child before age 30 and breastfeeding for at least six months can also reduce risk. At the Texas Breast Center, we provide comprehensive advice and support to help you understand and manage all known risk factors for breast cancer.
How does having a BRCA1 or BRCA2 mutation affect my breast cancer risk?
Having a BRCA1 or BRCA2 mutation significantly increases a person’s risk of developing breast and ovarian cancer. Regular screening mammograms, clinical oncology consultations, and preventive healthcare measures, such as risk-reducing surgeries (e.g., having your ovaries removed), are essential for individuals with these genetic mutations. The Texas Breast Center provides personalized care and support for individuals with BRCA1 or BRCA2 mutations to help manage their increased risk.
Does taking certain medications like aromatase inhibitors or letrozole affect my breast cancer risk?
Aromatase inhibitors and letrozole are medications used to reduce the risk of breast cancer recurrence in postmenopausal women with hormone receptor-positive breast cancer. While these medications can reduce the risk of breast cancer recurrence, they can have side effects such as symptoms of menopause, edema, and bone loss. It’s essential to discuss the benefits and risks of these medications with your healthcare provider at the Texas Breast Center.
Breast cancer, a predominant concern in women’s health, has roots traced to an array of causes and risk factors. One of the key risk factors is found in the complex relationship between hormones and the development of breast cancer. This intricate connection plays a vital role in understanding the disease and managing potential risks. At Texas Breast Center, under the proficient guidance of Dr. Gorman, the mission remains unwavering – to offer patients an advanced, personalized, and targeted approach to breast surgery and the treatment of breast cancer. Embracing evidence-based methodologies, the center keeps abreast of current research, including data from prominent organizations like the American Cancer Society, Cancer Research UK, and National Cancer Institute, to understand the hormonal risks associated with breast cancer. Through this article, readers will be enlightened about the role of hormones, from estrogen levels and aromatase inhibitors to hormone replacement therapy (HRT), and the impact of birth control pills in influencing breast cancer risk factors. Given the importance of health equity and patient-centric care, Dr. Gorman’s approach ensures that every patient is informed, empowered, and equipped to make the best treatment decisions.
This comprehensive article will delve deep into the correlation between breast cancer causes and hormone-related risks. The significance of this article is not just in understanding risks but also in appreciating preventive measures that can save lives. So, let’s embark on this journey to enhance our knowledge, guided by the expertise of Dr. Gorman and the legacy of care at the Texas Breast Center.
Estrogen Exposure
Estrogen, a paramount sex hormone in the female body, not only oversees a woman’s sexual development but also has profound implications on her breast health. The interplay between estrogen and breast cancer risk factors is underscored by research published in journals like The National Cancer Institute. It’s essential to delve deep into various facets of estrogen exposure to appreciate their implications.
Early Menstruation
Women who commence their menstrual cycle at an earlier age find themselves at the forefront of prolonged estrogen exposure. Initiating menstruation before the age of 12 has been linked to a slightly higher risk of breast cancer than those who begin after 14. As cancer research suggests, this prolonged exposure increases breast cell proliferation, sometimes leading to mutations and thereby increasing breast cancer risk. On the flip side, women who experience a late menopause continue to produce estrogen naturally beyond the average age, potentially increasing their risk further.
Late Menopause
Late menopause, which refers to the cessation of the menstrual cycle after the age of 55, further extends the period during which a woman’s body is exposed to estrogen. With the ovaries producing estrogen for a more extended period than average, these women have a heightened risk. There is a great deal of breast cancer research available that reveals a direct correlation between late menopause and a slight increase in the vulnerability to breast cancer.
Hormone Replacement Therapy and Certain Oral Contraceptives
Hormone replacement therapy (HRT), especially combined HRT containing estrogen and progesterone, is often prescribed to relieve symptoms of menopause, like vaginal dryness and hot flashes. However, certain types of HRT, particularly those with a combination of estrogen and progestogen, have been associated with an increased risk of breast cancer. Oral contraceptives, commonly known as birth control pills, also play a role. According to the American Cancer Society, using combined oral contraceptive pills may result in a modest increase in risk, though the risk tends to return to normal over time after discontinuing the pills. It’s imperative to note that the landscape of HRT and breast cancer is continually evolving, with research such as the Women’s Health Initiative shedding more light on this intricate relationship.
Delving into the realm of estrogen exposure underscores the importance of women being informed about their choices, whether related to birth control or menopause relief options. Dr. Gorman at the Texas Breast Center remains committed to equipping her patients with the information they need to navigate these decisions, drawing from worldwide epidemiological evidence and the latest cancer research.
Progesterone Exposure
Progesterone, another pivotal sex hormone in women, is instrumental in regulating the menstrual cycle and maintaining the early stages of pregnancy. While its role in the body is crucial, there’s also an undeniable link between progesterone and breast cancer risk.
Hormone replacement therapy (HRT) has long been a beacon of relief for postmenopausal women, alleviating symptoms like osteoporosis and certain menopausal symptoms. However, combined HRT, which contains both estrogen and progesterone (or a synthetic version called progestogen), has come under scrutiny for its potential risks. Evidence from the Women’s Health Initiative and other cohort studies points to a significant finding: combined HRT can increase breast cancer risk compared to estrogen-only therapy.
In fact, studies show how the inclusion of progesterone in therapy might boost the risk of breast cancer growth. It’s believed that progesterone can stimulate breast cell division, a process that might inadvertently increase the likelihood of DNA mistakes, eventually leading to cancer. When juxtaposed with estrogen, this combined effect potentially heightens the risk further.
Moreover, according to a systematic review in The Lancet, even women taking oestrogen-only HRT for more than five years post-menopause exhibited an elevated risk of breast cancer. But it’s the combination, with progesterone, that remains more concerning. While combined HRT’s benefits can be substantial for some women, understanding the potential risks is of paramount importance.
The narrative around progesterone exposure and breast cancer risk magnifies the need for informed decisions regarding HRT. Dr. Gorman’s approach at the Texas Breast Center revolves around ensuring that every woman is equipped with comprehensive cancer information. The goal is to strike a balance between alleviating menopausal symptoms and ensuring optimal long-term health outcomes.
Pregnancy and Breastfeeding
Breast cancer, the nefarious disease that has long cast a shadow over women’s health, has a web of intricate factors influencing its manifestation. The collaborative group, including the Collaborative Group on Hormonal Factors in Breast Cancer, has worked tirelessly to shed light on some of these intricacies. Within this sphere, pregnancy and breastfeeding stand out as two key factors that interact with a woman’s risk of developing breast cancer.
Pregnancy’s Protective Effect
A woman’s journey through pregnancy results in numerous changes in her body, from hormonal shifts to alterations in breast tissue. Epidemiology studies, particularly cohort study designs, show that women who have had children, especially before the age of 30, have a lower risk of developing breast cancer than women who never gave birth. The exact reasons are intricate, but factors such as changes in hormone levels, particularly reduced lifetime exposure to estrogen, and changes in breast cells that make them more resistant to the changes that can lead to breast cancer, are believed to be crucial.
Another dimension to consider is the role of genes. While mutations like BRCA are popularly linked to a heightened breast cancer risk, paradoxically, these carriers see a temporary increase in breast cancer risk after pregnancy. However, after a couple of decades, pregnancy will have a protective effect, even for them. It’s crucial to be guided by a thorough understanding of family history and gene implications, especially when discussing the effects of pregnancy on breast cancer risk.
Breastfeeding and Its Influence
Breastfeeding is another facet of maternal health with implications for breast cancer. The American Cancer Society posits that women who breastfeed for several months might reduce their risk of developing breast cancer. Biologically, breastfeeding makes sense as a protective measure. Not only does it alter the balance of hormones in the body, potentially delaying menstrual cycles and hence reducing estrogen exposure, but it also leads to differentiation of breast cells, making them less susceptible to the carcinogen-induced transformations that result in cancer.
Furthermore, during breastfeeding, women often have fewer menstrual cycles, leading to a decrease in estrogen and progesterone levels, two sex hormones linked to certain types of breast cancers. The longer women breastfeed, the greater the protective effect. Breast tissue that has undergone the changes due to lactation has a lower propensity for carcinogenic transformation, emphasizing the protective role of breastfeeding.
To further complicate the relationship between breastfeeding, pregnancy, and breast cancer risk, one must consider other risk factors like body weight, behavior during pregnancy like drinking alcohol, and exposure to certain drugs, including antidepressant medications like celexa or citalopram. The Mayo Clinic, for example, has published insights on how alcohol consumption during pregnancy, even in moderate amounts, might elevate the risk for both the mother and the child.
In the intricate narrative of breast health, Dr. Gorman at the Texas Breast Center acknowledges that while pregnancy and breastfeeding can play protective roles, they are but pieces of a much larger puzzle. Every woman’s body and circumstances are unique, and these factors interplay differently. Through a combination of advanced screening techniques and patient-specific risk assessments, a more holistic understanding of individual risks can be achieved, ensuring that every woman has the most accurate cancer information and the best care options available to her.
Obesity
In recent decades, there’s been a significant shift in global health dynamics with obesity emerging as a chief concern, affecting millions worldwide. The relationship between obesity and breast cancer is particularly important, not just because of the scale of the obesity epidemic but due to the intricate ways in which adipose tissue, commonly known as fat tissue, plays a role in hormone regulation.
The Connection Between Obesity and Breast Cancer Risk
Post-menopause, a woman’s ovaries cease to be the primary estrogen production site; instead, this role is overtaken by the adipose tissue. Elevated body weight, particularly in postmenopausal women, signifies a higher volume of adipose tissue. This, in turn, translates to higher estrogen production, which has been shown in numerous studies, including those in cancer epidemiol biomarkers prev and br j cancer, to correlate with an increased breast cancer risk.
Obesity is also associated with higher levels of insulin and insulin-like growth factor-1 (IGF-1) in the blood, two elements known to fuel breast cancer growth. The Cancer prevention initiatives by the American Cancer Society highlight the link between these elevated blood factors and the development of certain cancers, including breast cancer.
Moreover, fat cells produce adipokines, hormones that might stimulate or inhibit cell growth. For instance, leptin, which is more abundant in obese individuals, seems to promote cell proliferation, a key factor in cancer development.
Nuanced Implications of Obesity on Breast Cancer Type
While obesity increases the risk for hormone receptor-positive breast cancers in postmenopausal women, its impact on triple-negative breast cancer or other breast cancer types remains more elusive. Some studies, such as those conducted by the National Cancer Institute (natl cancer inst), have indicated a potential link between obesity and more aggressive forms of breast cancer, but these findings need more comprehensive validation.
Counteracting the Obesity-Driven Risk
While the connection between obesity and increased breast cancer risk is evident, the silver lining is that it’s a modifiable risk factor. Adopting a healthy weight regime, incorporating a balanced diet, and eschewing behaviors that contribute to weight gain can significantly lower the risk. The relay for life initiative, as well as efforts from cancer centers across the United States and the United Kingdom, underscore the importance of maintaining a healthy weight as an essential component of cancer care and prevention.
In conclusion, understanding the nuanced relationship between obesity and breast cancer is paramount. Dr. Gorman at the Texas Breast Center underscores the importance of maintaining a healthy weight, especially post-menopause, as a proactive measure against breast cancer. The center offers a multidimensional approach, combining risk assessments, adjuvant therapies, and personalized guidance to aid patients in navigating the complexities of obesity-related breast cancer risks.
Hormone Receptor Status
Hormone receptor status is a critical biomarker in breast cancer diagnosis, dictating not only the nature of the cancer but also influencing treatment options and overall prognosis. Understanding this status is essential for patients and their healthcare providers to make informed decisions about cancer care.
What is Hormone Receptor Status?
In the realm of breast cancer, hormone receptor status pertains to whether or not cancer cells have receptors that bind to certain hormones, predominantly estrogen and progesterone. When these receptors are present, the hormones can fuel breast cancer growth. The key receptors are:
Estrogen Receptor (ER): Breast cancers with these receptors are labeled as ER-positive. Estrogen, a naturally occurring hormone in the human body, can attach to these receptors, promoting the proliferation of cancer cells.
Progesterone Receptor (PR): Similarly, if the breast cancer cells have receptors for progesterone, they are termed PR-positive. When progesterone attaches to these receptors, it can stimulate the cancer cells to grow.
The presence or absence of these receptors provides pivotal insights into the behavior of the cancer and potential treatment avenues. For instance, ER-positive or PR-positive breast cancers can often be treated with hormone-blocking therapies like tamoxifen or aromasin.
Triple-Negative Breast Cancer
On the other end of the spectrum lies triple-negative breast cancer, a type which tests negative for estrogen receptors, progesterone receptors, and excess HER2 protein. This cancer type is particularly aggressive and lacks the targeted treatments that hormone receptor-positive cancers benefit from. Studies in journals like breast cancer res treat and cancer epidemiol biomarkers have extensively profiled the challenges and potential therapeutic avenues for triple-negative cases.
Testing and Implications for Treatment
Typically, the hormone receptor status is identified through tests conducted on tissue samples, often after a biopsy or surgery. The results can then guide treatment decisions. For instance, ER-positive breast cancers might be treated with drugs like tamoxifen, which blocks estrogen from binding with the receptors. On the other hand, triple-negative breast cancers might require a combination of surgery, radiation therapy, and chemotherapy.
It’s also worth noting the importance of understanding a patient’s entire clinical picture, including other risk factors such as family history, genetic markers like BRCA mutations, and environmental factors. The collaborative group on Hormonal Factors in Breast Cancer, for instance, has pooled data from various cohort studies and case–control study initiatives to provide a comprehensive understanding of how these diverse elements interplay with hormone receptor status.
The Texas Breast Center’s Approach
The Texas Breast Center stays at the forefront of understanding the intricacies of hormone receptor status. Utilizing state-of-the-art technology and collaborative efforts, the center ensures precise diagnosis, which is the first step towards personalized and targeted treatment options. Moreover, patients are provided with related information, resources, and support to navigate their journey with confidence.
In essence, understanding the hormone receptor status is not just about categorizing the cancer but tailoring the most effective treatment plan for each individual. This personalized approach translates to better breast cancer survival rates and improved quality of life for patients.
Empowering the Future: The Way Forward in Understanding Hormone-Related Breast Cancer Risks
Breast cancer, a diverse and multifaceted disease, is deeply intertwined with hormonal and various other factors. From the vulnerability disclosure of adipose tissue playing a role in estrogen production to the meta-analysis of breast cancer survival rates, it’s evident that knowledge and research are our strongest allies in combating this condition.
The importance of understanding hormone-related breast cancer causes cannot be understated. Data from the American Cancer Society’s cancer statistics and journals like J Natl Cancer Inst and Br J Cancer constantly illuminate the relationship between the human body and the risk of developing breast cancer. Both endogenous hormones and external factors, such as diet and behavior, affect breast tissue and can lead to disease.
Moreover, it’s imperative to consider the role of drugs, from antidepressants like celexa and sertraline to selective serotonin reuptake inhibitors, as they may have implications for breast cancer risk. Similarly, certain cancers like colorectal cancer, uterine cancer, and ovarian cancer have shared risk factors, emphasizing the need for a holistic approach to cancer prevention and treatment.
The benefits of an advanced, personalized, and targeted approach to breast surgery and the treatment of breast cancer at the Texas Breast Center are many-fold. From ensuring patients are at a healthy weight to providing palliative care, the center stands as a beacon of hope for many. Their innovative strategies, rooted in the latest research from collaborative groups and pooled analysis studies, serve as a testament to their commitment to excellence.
Cancer screening, early detection, and relay for life programs are pivotal to lowering the risk and improving breast cancer survival rates. Moreover, the role of the patient cannot be emphasized enough. Being informed about signs and symptoms, understanding one’s hormone receptor status, and seeking timely consultation can make a world of difference.
In the battle against breast cancer, knowledge truly is power. Whether it’s understanding the effects of diet and body weight, the impact of certain medications, or the genetic factors like BRCA that can increase risk, every piece of information paves the way for better outcomes.
Our call to action is clear: stay informed, be proactive, and seek consultation when in doubt. The Texas Breast Center stands ready to guide, support, and treat, ensuring every patient has the best chance at a healthy future.
See the other articles in the Causes series, including Age-Related Risks.
Frequently Asked Questions About Hormone-Related Risks
Can hormone therapy and breast implants increase my risk for breast cancer?
Yes, hormone replacement therapy (HRT), particularly the combination of estrogen and progestin, has been linked to increased risks of breast cancer. However, the risk varies depending on the type of HRT taken. Estrogen-only HRT carries a slight decrease in risk, while combined estrogen and progestin HRT increases breast cancer risk. Breast implants have been associated with a rare type of non-Hodgkin’s lymphoma called breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), but more research is needed to confirm the relationship between breast implants and breast cancer. At Texas Breast Center, we offer personalized consultations to discuss your individual risks and the best approach for your care.
How does being overweight or obese affect my risk for breast cancer?
Carrying excess body weight has been linked to an increased risk of postmenopausal breast cancer. This is because fat tissue, or adipose tissue, produces estrogen, and higher levels of estrogen can fuel breast cancer growth. Moreover, overweight or obese individuals often have higher levels of insulin and inflammation, which may also contribute to an increased risk of cancer. Managing body weight through a healthy diet and regular exercise can help lower the risk. At the Texas Breast Center, we provide guidance on maintaining a healthy weight as part of a comprehensive approach to breast health.
What is the relationship between hormone receptor status and breast cancer?
Hormone receptor status refers to the presence of receptors for the hormones estrogen and progesterone on the surface of cancer cells. Breast cancers that have these receptors are classified as hormone receptor-positive (estrogen receptor-positive and/or progesterone receptor-positive) and can be treated with hormone-blocking therapies. On the other hand, triple-negative breast cancers do not have estrogen, progesterone, or HER2 receptors and require different treatment approaches. Understanding the hormone receptor status of breast cancer is crucial for determining the most effective treatment strategy. At Texas Breast Center, we use advanced testing to determine the hormone receptor status and tailor the treatment accordingly.
What is the impact of hysterectomy and ovarian function on breast cancer risk?
Hysterectomy (removal of the uterus) and oophorectomy (removal of the ovaries) can impact breast cancer risk by altering the levels of sex hormones in the body. A hysterectomy alone does not significantly affect breast cancer risk, but removing the ovaries reduces the production of estrogen and progesterone, which can lower the risk of developing breast cancer, particularly for women with a BRCA1 or BRCA2 mutation. However, this comes with an increased risk of other health issues, such as osteoporosis and heart disease. At Texas Breast Center, we carefully evaluate all options to provide a personalized recommendation based on your individual risks and overall health.
Can taking certain drugs, like Tamoxifen, reduce my breast cancer risk?
Yes, Tamoxifen is a drug that blocks the estrogen receptors on breast cells, thereby helping to reduce the risk of hormone receptor-positive breast cancer in both premenopausal and postmenopausal women. Other drugs, such as raloxifene and aromatase inhibitors, can also reduce the risk of certain types of breast cancer. However, these drugs come with potential side effects and are not suitable for everyone. It is important to discuss the benefits and risks of these medications with your healthcare provider. At Texas Breast Center, we consider all available options to recommend the most appropriate risk-reduction strategy for you.
How does menopausal status affect breast cancer risk and what role does hormonal contraception play?
Menopausal status is a significant factor in breast cancer risk. Pre-menopausal women have a lower risk compared to post-menopausal women. The use of hormonal contraception, which includes combined oestrogen and progestin, can slightly increase the risk of developing breast cancer. However, the risk decreases after stopping hormonal contraception and eventually returns to that of the general population. At the Texas Breast Center, we can help you navigate the complexities of hormonal contraception and its implications on breast cancer risk.
Is there a link between endogenous sex hormones and breast cancer?
Yes, there is a well-established link between endogenous sex hormones, such as estrogen and progesterone, and breast cancer. High levels of these hormones in the blood have been associated with an increased risk of breast cancer in postmenopausal women. This is because estrogen and progesterone can stimulate the growth of breast cells, including cancer cells. Understanding your hormone levels and their impact on your breast cancer risk is an essential part of the personalized care we offer at the Texas Breast Center.
Can certain medications, like antidepressants, affect my breast cancer risk?
Some studies have suggested a potential link between the use of certain antidepressants, such as selective serotonin reuptake inhibitors (SSRIs) like citalopram, sertraline, and paroxetine (Paxil), and a slightly increased risk of breast cancer. However, the evidence is not conclusive, and more research is needed to confirm this association. It is important to weigh the benefits of antidepressants in managing depression and anxiety against any potential risks. At the Texas Breast Center, we consider all aspects of your health and work collaboratively with your healthcare team to provide the most comprehensive care.
Is there a genetic component to hormone-related breast cancer?
Yes, certain genetic mutations, such as those in the BRCA1 and BRCA2 genes, can increase the risk of hormone receptor-positive breast cancer. Women with these mutations have a higher risk of developing breast cancer at a younger age and are often recommended to undergo more frequent screening and consider risk-reduction strategies, such as prophylactic mastectomy or oophorectomy. Genetic testing and counseling are crucial components of the comprehensive care we provide at the Texas Breast Center.
Are there clinical trials available for hormone-related breast cancer?
Yes, there are ongoing clinical trials exploring new treatments and prevention strategies for hormone-related breast cancer. These trials may involve novel hormonal therapies, targeted therapies, or combination approaches. Participation in a clinical trial is a personal decision and may offer access to cutting-edge treatments that are not yet widely available. At the Texas Breast Center, we can help you understand your options and determine if a clinical trial is appropriate for your specific situation.
What is the relationship between ductal carcinoma in situ and hormone-related breast cancer?
Ductal carcinoma in situ (DCIS) is a non-invasive form of breast cancer that starts in the milk ducts (mammary glands) and has not yet spread to nearby tissues. Hormones, especially estrogen, can fuel the growth of some DCIS, making it hormone receptor-positive. Understanding the hormone receptor status of DCIS is crucial for determining the most effective treatment plan. At the Texas Breast Center, we provide comprehensive evaluation and personalized treatment plans for DCIS and other forms of breast cancer.
Can feminizing hormone therapy increase the risk of breast cancer?
Feminizing hormone therapy, which often includes estrogen and Medroxyprogesterone acetate, is used by transgender women and non-binary individuals assigned male at birth who are undergoing gender transition. There is some evidence to suggest that feminizing hormone therapy may slightly increase the risk of breast cancer, although the overall risk remains relatively low. It is important to have regular breast cancer screenings and discuss any concerns with your healthcare provider. At the Texas Breast Center, we provide inclusive and personalized care for all individuals.
Is there a link between endometrial cancer and breast cancer?
Yes, there is a link between endometrial cancer (cancer of the lining of the uterus) and breast cancer. Both cancers share common risk factors, such as obesity, hormone replacement therapy (HRT), and a family history of these cancers. Additionally, some genetic mutations, such as those in the BRCA1 and BRCA2 genes, increase the risk of both breast and endometrial cancers. At the Texas Breast Center, we provide comprehensive genetic testing and counseling to assess your risk for multiple types of cancer.
What is the role of randomized controlled trials in breast cancer research?
Randomized controlled trials (RCTs) are the gold standard in clinical research and play a crucial role in advancing our understanding of breast cancer and developing new treatments. In an RCT, participants are randomly assigned to receive either the experimental treatment or a standard treatment (or placebo), and the outcomes are compared. This design helps minimize bias and provides the most reliable evidence of a treatment’s effectiveness. At the Texas Breast Center, we actively participate in clinical trials and can help you determine if participation in a trial is appropriate for you.
What are the main risk factors for breast cancer?
The main risk factors for breast cancer include being female, increasing age, a family history of breast cancer, certain genetic mutations (e.g., BRCA1, BRCA2), a history of breast cancer or certain non-cancerous breast diseases, exposure to estrogen (e.g., hormone replacement therapy, late menopause, early menstruation), obesity, and lack of physical activity. Other factors, such as alcohol consumption, radiation exposure, and having dense breasts, can also increase risk. At the Texas Breast Center, we provide comprehensive risk assessment and personalized prevention strategies.
Does having ovarian cancer affect the relative risk of developing breast neoplasms related to hormone exposure?
Yes, having ovarian cancer can affect the relative risk of developing hormone-related breast neoplasms. The ovaries produce the majority of estrogen in premenopausal women, and alterations in ovarian function can lead to changes in hormone levels. Estrogen exposure is a well-established risk factor for breast cancer, and conditions that affect estrogen production, like ovarian cancer, can modify the relative risk of developing breast neoplasms. It’s crucial to monitor and manage hormone levels in women with ovarian cancer. At Texas Breast Center, we provide comprehensive care to assess and manage hormone-related risks for breast cancer.
Breast cancer, a widespread condition that affects millions of people worldwide, is not indiscriminate. Its incidence and course are shaped by a myriad of factors—genetic predispositions, environmental exposures, lifestyle choices, and more. Yet, among these various influences, one factor plays an especially profound role: gender.
This disease does not see all genders as equal. It selects, discriminates, and alters its strategies based on the gender of the individual it targets. Women, due to their unique biological and hormonal makeup, have a substantially higher risk of developing breast cancer. Meanwhile, men, while less likely to face the disease, often confront more advanced forms of it due to later diagnoses. These gender-related risks and outcomes are not just statistical quirks. They are critical dimensions of the disease that shape the way we approach prevention, screening, diagnosis, and treatment.
At the Texas Breast Center, Dr. Valerie Gorman and her expert team recognize and address these gender-influenced nuances of breast cancer. Their approach is rooted in the belief that understanding and respecting the distinctive aspects of each patient—including gender-specific factors—can lead to more precise diagnoses, more personalized treatments, and, ultimately, better health outcomes.
In the spirit of this commitment, this article delves into the gender-influenced causes and risk factors of breast cancer. It explores how the female and male genders, with their unique hormonal profiles and breast tissue compositions, interact differently with the disease. This exploration will not only deepen our understanding of breast cancer but also reaffirm the importance of a personalized, gender-conscious approach to tackling this challenging disease.
Gender-related Risk Factors
As we delve deeper into our discussion on breast cancer causes, it is imperative to focus on one of the most significant contributors – gender. In the complex landscape of risk factors that shape the occurrence and progression of breast cancer, gender holds a key position. It influences not only the likelihood of developing the disease but also the way it presents and progresses. This section aims to illuminate how the female and male genders, each with their unique hormonal environment and breast tissue composition, interact differently with breast cancer. By understanding these gender-related risk factors, we can promote more tailored prevention strategies and treatment plans, which is at the heart of the personalized approach of Dr. Gorman and her team at the Texas Breast Center.
Female Gender
When it comes to the occurrence of breast cancer, it is indisputable that women bear a disproportionately higher risk. This heightened susceptibility is largely due to the distinctive hormonal environment and the specific composition of female breast tissue.
Hormones, particularly estrogen and progesterone, have a crucial role in women’s reproductive health. However, their influence extends beyond fertility and has a significant bearing on the development of breast cancer. Longer lifetime exposure to these hormones, either due to early menstruation (before the age of 12) or late menopause (after the age of 55), can increase a woman’s risk of breast cancer.
Moreover, the anatomical and physiological characteristics of female breast tissue further contribute to this risk. The breast tissue in women is mostly composed of dense glandular and fibrous tissue, which not only makes tumors harder to detect but also increases the probability of cancerous changes.
Male Gender
In comparison to women, men have a significantly lower risk of breast cancer – less than 1% of all breast cancers occur in men. However, this reduced incidence should not encourage complacency. Men can and do get breast cancer. It is often diagnosed at a later stage in men due to lower awareness, resulting in less frequent screening and a lack of emphasis on self-examinations.
The anatomy of male breast tissue, being less dense, often means that tumors can be more easily palpated. Yet, a lack of awareness about male breast cancer can delay diagnosis, leading to a potentially poorer prognosis. This highlights the importance of education and awareness, a commitment that Dr. Gorman and her team at Texas Breast Center stand by, ensuring all patients, regardless of their gender, receive personalized and comprehensive care.
Hormonal Influences
Within the realm of gender-related risk factors, hormonal influences take center stage. Hormones, the body’s chemical messengers, hold significant sway over our health, including the development and progression of diseases like breast cancer. This section will delve into the specific roles of estrogen and testosterone – hormones that are differentially present in males and females – in the context of breast cancer risk. By shedding light on these intricate hormonal dynamics, we aim to enhance the understanding of these complex interactions, enabling healthcare providers like Dr. Gorman and the team at Texas Breast Center to devise treatment plans that are as individualized as the patients they serve.
Estrogen
Estrogen is a hormone that not only regulates the development of secondary sexual characteristics in women but also plays a pivotal role in breast cancer development. A woman’s risk of developing breast cancer is linked to her exposure to estrogen throughout her life. As mentioned before, early onset of menstruation and late menopause result in prolonged exposure to estrogen, thus increasing breast cancer risk.
Furthermore, the use of hormone replacement therapy (HRT), particularly therapies that include both estrogen and progesterone, has been associated with an increased risk of breast cancer. The risk appears to increase the longer a woman uses HRT and decreases over time once she stops using these medicines.
Testosterone
While the primary focus in the realm of breast cancer and hormones often falls on estrogen and progesterone, testosterone also plays a critical role. In men, lower levels of testosterone have been proposed as a possible factor in the development of breast cancer. Testosterone, a hormone present in both men and women, but in much higher levels in men, has a protective role against breast cancer. Thus, lower levels of testosterone might increase the risk of breast cancer in men. However, research in this area is still emerging, and a conclusive link has not been definitively established.
Texas Breast Center: Your Partnership for Personalized Breast Health Care
Understanding the interplay of gender and hormones in the development and progression of breast cancer is vital in developing effective preventive strategies and treatment plans. It underscores the importance of a personalized approach to breast health, taking into account the unique circumstances and risk factors inherent to each patient.
At the Texas Breast Center, Dr. Gorman and her team remain steadfastly committed to providing advanced, personalized, and targeted breast cancer care. Emphasizing patient education, early detection, and state-of-the-art treatment options, their approach ensures the highest standard of care for every patient, irrespective of gender.
Being proactive about breast health is essential. Regardless of your gender, understanding your unique risk factors, including how hormones influence your breast cancer risk, can be a life-saving decision. The team at the Texas Breast Center, led by Dr. Valerie Gorman, is here to guide and support you on this journey.
Schedule your personalized consultation today. Let’s work together on a plan to prioritize your breast health, monitor for changes, and, if needed, develop a targeted treatment strategy that suits your specific needs. At Texas Breast Center, you’re not just a patient; you’re part of a compassionate community committed to overcoming breast cancer together.
FAQ’s about Breast Cancer Causes: Gender Influencing Causes
What role does gender play in breast cancer risk?
Gender is one of the most significant factors influencing breast cancer risk. Women, due to longer exposure to female hormones and the nature of their breast tissue, have a higher risk of developing breast cancer. However, while men have a lower risk, when they do develop breast cancer, it’s often diagnosed at a later stage due to less awareness and infrequent screening.
How does estrogen affect breast cancer risk?
Estrogen, a hormone predominant in women, stimulates breast cell growth, including potentially cancerous cells. Prolonged exposure to estrogen, such as early menstruation, late menopause, or use of hormone replacement therapy, can increase a woman’s risk of breast cancer.
Can men get breast cancer?
Yes, men can get breast cancer, although it is much less common. Male breast cancer accounts for less than 1% of all breast cancer cases. Lower awareness and screening often result in later-stage diagnoses, emphasizing the importance of awareness in men too.
How does testosterone impact breast cancer risk?
Testosterone, primarily a male hormone but also present in women, has a protective role against breast cancer. Lower levels of testosterone might increase breast cancer risk, particularly in men. However, more research is needed in this area to establish a definitive link.
Are women who have never given birth at higher risk of breast cancer?
Yes, women who have never given birth, often referred to as nulliparous women, may have a slightly higher risk of breast cancer compared to women who have had one or more children. This is believed to be due to the longer uninterrupted exposure to estrogen and progesterone hormones that occurs in women who have not been pregnant.
Why is breast cancer usually diagnosed at a later stage in men?
Breast cancer is often diagnosed at a later stage in men primarily due to lower awareness and less frequent screening. Since breast cancer is less common in men, they might not be vigilant about noticing changes in their breasts and seeking prompt medical attention.
Does hormone replacement therapy (HRT) increase the risk of breast cancer?
Yes, hormone replacement therapy, particularly combined estrogen-progesterone therapy used after menopause, can increase the risk of breast cancer. The risk increases the longer a woman uses HRT and decreases over time once the usage stops.
How does early menstruation or late menopause increase breast cancer risk?
Early menstruation (before age 12) or late menopause (after age 55) can increase a woman’s risk of breast cancer. Both conditions result in a longer lifetime exposure to estrogen and progesterone, hormones that can stimulate the growth of breast cancer cells.
Is breast cancer in men as serious as in women?
Yes, breast cancer in men is as serious as in women. In fact, due to lower awareness and delayed diagnoses, it can often be more advanced when detected. Men need to be vigilant about noticing any changes in their breast tissue and should seek medical advice promptly if they do.
Do birth control pills increase the risk of breast cancer?
Some research suggests that current or recent use of birth control pills with high doses of estrogen can slightly increase the risk of breast cancer. However, this risk appears to go back to normal over time once the pills are stopped.
Does breastfeeding affect the risk of breast cancer?
Breastfeeding can slightly lower breast cancer risk, particularly if it’s continued for 1.5 to 2 years. This could be due to the fact that breastfeeding reduces a woman’s total number of menstrual cycles, and thus her lifetime exposure to estrogen.
Is the risk of breast cancer the same for all women?
No, the risk of breast cancer varies greatly among women due to differences in genetic factors, lifestyle choices, reproductive factors, and exposure to estrogen.
Does male breast cancer have the same symptoms as female breast cancer?
Yes, the symptoms of male breast cancer are similar to those in women. They include a lump in the breast, changes to the skin or nipple, and discharge from the nipple. However, any change in the chest area or breasts should prompt a doctor’s visit.
Does menopause affect the risk of breast cancer?
Postmenopausal women have a higher risk of breast cancer, primarily due to longer lifetime exposure to estrogen and progesterone. However, the risk declines over time after menopause as hormone levels decrease.
Can lifestyle changes reduce the risk of breast cancer in both men and women?
Yes, lifestyle changes such as maintaining a healthy weight, staying physically active, limiting alcohol intake, and eating a balanced diet can help reduce the risk of breast cancer in both men and women. It’s always advisable to discuss lifestyle changes with your healthcare provider.
Can hormone therapy be used in treating breast cancer in men?
Yes, hormone therapy can be used in treating breast cancer in men, especially for those with hormone-receptor positive tumors. This type of treatment blocks the cancer cells from getting the hormones they need to grow. However, the specific treatment approach is highly individualized, so patients should discuss their options with their healthcare provider.
Are there genetic factors that increase the risk of breast cancer in both men and women?
Yes, genetic mutations, most commonly in the BRCA1 and BRCA2 genes, can significantly increase the risk of breast cancer in both men and women. These mutations can be inherited from either parent and they increase the risk of both male and female breast cancers.
How does breast cancer form, and what are some of its advanced stages?
The landscape of breast cancer, a leading health concern globally, is intricate and complex. Every breast cancer case is unique and depends on an interplay of biological, genetic, environmental, and lifestyle factors. Breast cancer arises when breast cells become abnormal and multiply uncontrollably, forming a tumor. If not caught early, these cancerous cells can invade other parts of the body, leading to advanced cancers, which can be challenging to manage.
What are the structural elements of the female breast and how can changes in these tissues lead to breast conditions or cancer?
The female breast is composed primarily of fatty, or adipose tissue, and glandular tissue, which produces milk. Changes in these tissues, often influenced by hormonal variations, can lead to benign breast conditions such as atypical hyperplasia or potentially malignant ones like ductal carcinoma in situ (DCIS) or lobular carcinoma in situ (LCIS).
How do female hormones, particularly estrogen and progesterone, and male hormones like testosterone influence the risk of breast cancer
Female hormones, particularly estrogen and progesterone, play significant roles in both benign breast diseases and breast cancer. A woman’s risk of developing breast cancer increases with prolonged exposure to estrogen, such as early menstruation, late menopause, or use of hormone replacement therapy (HRT). Testosterone, a male hormone, is also implicated in breast cancer. In males, lower testosterone levels might be linked to an increased risk of breast cancer, a less common but equally serious condition. Men who have Klinefelter syndrome, a condition characterized by an additional X chromosome resulting in lower levels of testosterone and higher levels of estrogens, are at an elevated risk for developing male breast cancer.
What roles do specific genes, like BRCA1 and BRCA2, play in breast and ovarian cancer risk?
Specific genes, most notably BRCA1 and BRCA2, are known to increase the risk of both breast and ovarian cancer when mutated. These mutations can be inherited from either parent, and individuals with these mutations often require more aggressive screening and preventive measures. BRCA1/2 mutations can lead to hereditary breast cancer, which accounts for a significant fraction of breast cancer cases.
How does breast cancer screening work and what are some of its challenges?
Breast cancer screening, including mammography, aims at identifying breast cancer at an early stage when it is more treatable. While mammography has significantly improved breast cancer diagnosis, it’s not flawless. For instance, women with dense breast tissue often require additional imaging due to the increased difficulty of detecting tumors in dense breasts.
How do environmental factors, such as alcohol and radiation exposure, impact the risk of developing breast cancer?
Environmental factors, including alcohol and radiation exposure, have also been associated with an increased risk of breast cancer. Regular consumption of alcoholic beverages can heighten the risk, with heavy drinking or alcoholism posing a significant risk. Exposure to radiation, especially at a young age, also boosts the risk of developing breast cancer.
What lifestyle and behavioral factors contribute to the overall breast cancer risk?
In addition to these apparent risk factors, lifestyle and behavior are crucial components in the overall breast cancer risk. A diet high in processed and fatty foods, smoking, a sedentary lifestyle, and obesity can all amplify the risk of breast cancer. On the other hand, maintaining a healthy weight, regular physical activity, and breastfeeding can help reduce the risk.
What are some of the medical treatments for managing breast cancer, and how do they improve patient outcomes?
Finally, medical treatments, including certain types of chemotherapy, radiation therapy, endocrine therapies, antiandrogen therapy, and surgery, are all integral parts of breast cancer management. Adjuvant therapies, treatments given after the primary treatment to lower the chance of the cancer returning, can significantly improve survival rates in breast cancer patients.
How does precision in diagnosis and the right treatment plan impact patient outcomes?
Accurate and precise diagnosis, along with the right treatment plan, can greatly improve the outcome for a patient diagnosed with breast cancer. Moreover, advances in the field of cancer biomarkers and cancer research are paving the way for more personalized treatment approaches.
How are organizations like the American Cancer Society contributing to the fight against breast cancer?
The American Cancer Society, along with other global cancer initiatives, is dedicated to funding and conducting research to reduce the impact of breast cancer. From enhancing data collection to developing effective cancer programs, the fight against breast cancer is a collaborative effort involving healthcare professionals, researchers, corporate partners, and patients.
What role does the Texas Breast Center play in breast health awareness and patient care?
At the Texas Breast Center, we believe that education is a critical part of this fight. Our mission is to promote breast health awareness and provide the most advanced care to our patients. The journey to health equity begins with understanding, and we are here to guide you through it.
How important is individual risk assessment and early detection in breast cancer management?
While this article provides an overview of breast cancer causes and risk factors, remember that each individual’s risk is unique. If you have any questions or concerns about your breast health, reach out to a healthcare professional. It’s important to remember that early detection saves lives, and regular breast cancer screening according to guidelines can help ensure early detection.
Dr. Gorman’s unwavering commitment to delivering unmatched and customized healthcare consistently leads the way in comprehending the complex nature of breast cancer. Our primary goal at Texas Breast Center is to foster an informed community, one that is equipped with the knowledge needed to prevent, detect, and address breast cancer efficiently. It’s with this vision that we delve into the topic of “Breast Cancer Causes: Age Related Risks.”
Breast cancer is a complex disease with a myriad of contributing factors. Among these, age stands as a significant determinant. Despite the prevalence of breast cancer in younger women, it’s important to note that the risk indeed increases as women get older.
In this article, we’ll explore the reasons why age is a risk factor, the mechanisms behind this link, and provide practical advice on how women of all ages can monitor their breast health effectively.
This article embodies Dr. Gorman’s commitment to offering an advanced and targeted approach to breast health. Our aim is not just to treat but to educate, empower, and encourage women to take an active role in their health journey. Our hope is that through this understanding, we can collectively reduce the impact of breast cancer and improve the lives of women across Texas and beyond.
We invite you to take this journey with us, one step at a time, toward a future where knowledge and proactive actions make a significant difference in the fight against breast cancer.
Increasing age
Breast cancer risk is intrinsically linked with age, with an increased probability of developing the disease as women get older. This is primarily due to the cumulative effect of several risk factors over time, including exposure to estrogen, genetic mutations, and the natural wear and tear process at the cellular level.
Estrogen exposure plays a significant role in breast cancer risk. This hormone is necessary for normal breast development, but it can also facilitate the growth of some types of breast cancer. Throughout a woman’s life, her body is exposed to varying levels of estrogen, primarily produced by the ovaries. Women who have had longer menstrual histories (i.e., those who started menstruating early and/or went through menopause late) have a slightly higher risk due to longer lifetime exposure to the hormone.
With increasing age, the likelihood of genetic mutations also increases. These mutations can accumulate over time due to various factors such as exposure to radiation, certain chemicals, and random errors that occur when cells divide. Some of these mutations can cause cells to become cancerous.
Moreover, the aging process naturally brings about a decline in the body’s immune function, reducing its ability to detect and destroy cells that have become abnormal, potentially leading to cancer.
While breast cancer can and does occur in younger women, it is less common. According to the American Cancer Society, the average risk of a woman developing breast cancer increases dramatically with age. Statistically, the majority of breast cancer cases are diagnosed in women over the age of 50. In fact, the median age for breast cancer diagnosis in the United States is 62, with most cases occurring in this age bracket. This is not to say that younger women should not be vigilant; rather, it underscores the importance of regular screenings, especially as women age.
Younger women
Breast cancer is relatively rare in younger women, with very few breast cancer cases in the U.S. being diagnosed in women under the age of 40, according to the American Cancer Society. This is due to several reasons, one being that breast tissue in younger women is denser, which may limit the effectiveness of mammography and lead to later detection. Moreover, younger women have fewer cumulative lifetime exposure to various risk factors like estrogen.
However, when breast cancer does occur in younger women, it tends to be diagnosed at a later stage and often presents as more aggressive forms of the disease. One reason for this is that breast cancer in younger women can be more difficult to detect due to the dense breast tissue, as mentioned before. This might delay diagnosis and consequently, treatment.
Moreover, younger women are more likely to have what is known as “triple-negative” breast cancer – a type of breast cancer that is particularly aggressive and less responsive to standard hormonal therapies. This subtype of cancer does not express the three most common types of receptors known to fuel breast cancer growth—estrogen, progesterone, and the HER-2/neu gene. Therefore, treatment options can be more limited and the cancer can be more challenging to treat successfully.
Another aggressive form that occurs more commonly in younger women is HER2-positive breast cancer, which is characterized by the overexpression of the HER2 protein. This form of breast cancer tends to grow and spread more quickly than other types.
It’s important to note that, regardless of age, any new or unexplained breast symptoms should be evaluated promptly by a healthcare professional. For younger women, especially those with a family history of breast cancer or other risk factors, proactive measures such as self-examinations, regular clinical exams, and discussions with healthcare providers about individual risk can contribute significantly to early detection and improved outcomes.
Age at first menstruation
The age at which a woman starts menstruating, also known as menarche, can indeed influence her risk of developing breast cancer later in life. Research indicates that women who experience their first period before the age of 12 have a slightly elevated risk of developing breast cancer compared to those who started menstruating at a later age.
This association primarily stems from the lengthened exposure to estrogen and progesterone – hormones that are known to stimulate breast cell growth. Simply put, the earlier a girl starts her periods, the longer her lifetime exposure to these hormones.
During each menstrual cycle, the levels of estrogen and progesterone in a woman’s body rise to prepare for a potential pregnancy. These hormonal surges stimulate the growth of the glandular tissue in the breasts. Although this is a natural process, over time, this increased cell activity raises the chances of a DNA error during cell division, potentially leading to cancerous mutations.
In addition, early menstruation usually means a longer time until menopause. Menopause is another significant event in a woman’s life when the ovaries stop producing eggs, and the production of estrogen and progesterone declines. Therefore, the longer time from menarche to menopause translates into more menstrual cycles, and subsequently, a longer cumulative exposure to estrogen and progesterone.
While the increased risk linked with early menarche is relatively small on an individual level, it’s significant from a public health perspective given the high prevalence of breast cancer. This connection underlines the importance of regular breast cancer screenings, especially for women who began menstruating at an early age.
Age at menopause
The age at which a woman reaches menopause also significantly influences her risk of developing breast cancer. Research suggests that women who experience menopause after the age of 55 have a slightly increased risk of breast cancer compared to women who reach menopause before the age of 45.
This heightened risk is predominantly due to prolonged exposure to hormones such as estrogen and progesterone, which are produced in a woman’s body during her reproductive years. These hormones have been associated with stimulating cell growth in the breasts, and prolonged exposure to them can increase the chance of DNA errors during cell division, which can result in cancerous mutations.
Late menopause means that a woman’s body continues to produce these hormones, and her breast tissue continues to be exposed to their growth-promoting effects for a longer duration. This cumulative hormonal exposure over many years increases the likelihood of developing breast cancer.
Moreover, the risk associated with late menopause might also be linked to the increased number of menstrual cycles a woman goes through in her lifetime. Each menstrual cycle is associated with a surge in estrogen and progesterone levels, which stimulate breast cell multiplication, potentially leading to errors in cell replication and an increased risk of mutation.
While the increased risk associated with late menopause is considered modest, it’s significant enough to warrant attention, especially considering the high incidence of breast cancer. Therefore, it is crucial for women who experience late menopause to engage in regular screenings and take proactive steps to reduce their breast cancer risk. These steps can include maintaining a healthy lifestyle, which involves regular physical activity, a balanced diet, limiting alcohol consumption, and avoiding tobacco.
Age at first full-term pregnancy
The age at which a woman has her first full-term pregnancy can influence her risk of developing breast cancer. Research has shown that women who have their first full-term pregnancy after the age of 30 have a slightly increased risk of developing breast cancer compared to women who have their first child before the age of 20.
This somewhat counterintuitive relationship between pregnancy and breast cancer risk is likely due to the complex interplay of hormonal changes that occur during pregnancy. Pregnancy induces significant changes in the levels of hormones such as estrogen and progesterone in a woman’s body, and these hormones have a profound impact on the cells of the breast.
During a first full-term pregnancy, the breasts undergo permanent cellular changes. Before this, the breast cells are immature and more susceptible to the carcinogenic effects of hormones and environmental toxins. A full-term pregnancy matures these cells, making them less likely to become cancerous.
However, this protective effect is more pronounced when the first full-term pregnancy occurs at a younger age. When the first full-term pregnancy occurs after the age of 30, the breast cells have had more time to accumulate genetic damage, which could potentially lead to cancer. Thus, the overall effect of a later first pregnancy might result in a net increase in breast cancer risk.
Moreover, during pregnancy, especially in the early stages, levels of estrogen increase, which leads to rapid growth of breast cells. This increased cell division can raise the risk of mutations and cancer development.
Despite this slight increase in risk, it’s important to note that the decision to have children and when to have them is personal and can be influenced by various factors. It’s just one of many factors that contribute to breast cancer risk, and having a first child after 30 does not guarantee one will develop breast cancer. As always, regular screenings and healthy lifestyle choices are key components in the proactive management of breast cancer risk.
Age at first childbirth
The age of a woman at the time of her first childbirth, or not having given birth at all, can influence her risk of developing breast cancer. Research indicates that women who never have a full-term pregnancy have a slightly higher risk of breast cancer compared to those who have their first child at a younger age.
One of the primary reasons behind this increased risk is the prolonged and uninterrupted exposure to estrogen and progesterone. These hormones are naturally produced during a woman’s menstrual cycle and have been associated with increased cell growth in the breasts. A woman who has never been pregnant has more menstrual cycles compared to a woman who has one or more pregnancies, thus increasing her cumulative lifetime exposure to these hormones.
During pregnancy, the breasts go through changes that make them more resistant to transformations that can lead to cancer. The cells of the breast differentiate, or specialize, to produce milk – a change that seems to make the breast cells less likely to undergo cancerous changes. An absent pregnancy means the breast tissue goes through fewer of these protective changes.
Additionally, the surge of hormones during pregnancy causes breast cells to rapidly divide and grow. While this is normal, increased cell division can also increase the chance of genetic mistakes or mutations, potentially leading to cancer. The risk of this occurring is higher in older women, as cells accumulate genetic changes over time.
It’s crucial to note that while these factors do contribute to an increased risk, it’s a relative increase and the overall risk remains modest. Not having children is a personal decision influenced by a wide range of factors. Regular breast cancer screenings and maintaining a healthy lifestyle remain the most effective strategies for all women to manage their individual risk.
Age at breast cancer diagnosis
While it’s true that breast cancer risk increases with age, the nature of the disease can vary based on the age at diagnosis. Generally, older women (especially those over 70) diagnosed with breast cancer tend to have a more favorable prognosis compared to younger women. This is, in part, due to the fact that breast cancers in older women often grow more slowly.
Cancer growth rate is significantly influenced by the characteristics of the cancer cells and the surrounding environment. Age-related changes in both the breast tissue and the body’s overall immune response can impact the rate at which a tumor grows.
Breast cancers in older women are often hormone receptor-positive, meaning that the cancer cells have receptors that attach to hormones like estrogen and progesterone. Hormone receptor-positive cancers tend to grow more slowly than cancers that are hormone receptor-negative. Moreover, treatments that block these hormones or their receptors can effectively slow or stop the growth of these cancers.
Furthermore, older adults often have a reduced immune response, which paradoxically, may slow the growth rate of the cancer. An aggressive immune response can sometimes stimulate cancer cells to grow and divide more rapidly, a phenomenon known as inflammation-induced tumor growth. The diminished immune response in older adults may limit this effect.
However, it’s important to note that although the prognosis may be generally better due to slower tumor growth, older women might face other challenges related to breast cancer management. These can include an increased risk of treatment side effects and the presence of other health conditions that might complicate care. Therefore, an individualized and comprehensive approach to treatment is crucial.
Finally, regardless of age, early detection remains the key to a more favorable prognosis in breast cancer. Regular screenings and understanding personal risk factors contribute significantly to early diagnosis and effective treatment.
Age-specific breast cancer rates
Breast cancer incidence rates do indeed vary by age group. It’s a well-established fact that the risk of developing breast cancer increases as women age. According to the American Cancer Society, women aged 70-74 generally have the highest incidence rates of breast cancer.
This trend can be attributed to several reasons. First, the process of aging itself results in an accumulation of genetic mutations over time due to factors like exposure to carcinogens, errors during DNA replication, and decreased efficiency of DNA repair mechanisms. These factors can eventually lead to the development of cancer.
Second, older women have had more menstrual cycles, resulting in a longer lifetime exposure to hormones such as estrogen and progesterone. These hormones, which are known to stimulate cell growth in the breasts, can over time lead to uncontrolled cell growth and potential transformation into cancer cells.
Third, as women age, they experience more instances of proliferative breast diseases with atypia, which are known risk factors for breast cancer. Atypia refers to the presence of abnormal cells, which are more likely to become cancerous.
Furthermore, the body’s immune system, which helps to detect and destroy abnormal cells, declines with age. This decline might allow some cancerous cells to multiply and form tumors before they’re detected by the immune system.
Despite the higher incidence rate in older women, it’s important to note that breast cancer can occur at any age, and younger women can also develop aggressive forms of the disease. Therefore, it’s crucial for women of all ages to understand their individual risk factors, including genetics, and engage in recommended screening practices for early detection of the disease. It’s also essential to maintain a healthy lifestyle, as several risk factors for breast cancer, such as maintaining a healthy weight and regular physical activity, are within an individual’s control.
Age-related hormone exposure
Estrogen and progesterone are hormones that are naturally produced in a woman’s body and play crucial roles in the menstrual cycle and pregnancy. However, longer lifetime exposure to these hormones has been associated with an increased risk of developing breast cancer.
This increased risk is predominantly due to the role these hormones play in cell growth. Both estrogen and progesterone stimulate the growth of cells in the breast — a normal process that facilitates the development and maintenance of the mammary glands in response to each menstrual cycle. However, with longer exposure to these hormones, there is an increased opportunity for the growth of cells in the breast. This increased cell division can potentially result in errors during the replication of DNA, which can, in turn cause mutations that may lead to cancer.
In essence, the longer the breast tissue is exposed to these hormones, the higher the chance that a breast cell could turn cancerous. Factors that can lengthen a woman’s exposure to these hormones include early menarche (starting menstruation before age 12), late menopause (experiencing menopause after age 55), late or no pregnancy, and certain types of hormone replacement therapy or birth control. Each of these conditions leads to a longer timeframe during which the breast tissue is exposed to estrogen and progesterone, thereby increasing the risk of breast cancer.
It’s also worth noting that not all breast cancers are hormone receptor-positive, meaning that not all breast cancers grow in response to estrogen or progesterone. Some types of breast cancer are hormone receptor-negative and grow independently of these hormones. Therefore, while it’s true that longer lifetime exposure to estrogen and progesterone increases the risk of breast cancer, it’s not the only factor at play.
Nevertheless, understanding this relationship underlines the importance of regular breast cancer screenings and lifestyle modifications where possible, to manage and mitigate the risk associated with prolonged hormone exposure.
Age and breast cancer screening
Mammograms, which are X-ray images of the breast, are an essential tool for the early detection of breast cancer. Regular mammogram screenings are typically recommended for women aged 40 and older, though the exact age to start and frequency of screenings can depend on individual risk factors and professional guidelines.
The primary aim of a mammogram screening is to identify breast cancer before any physical symptoms develop. Detecting cancer at an early stage often means that it is smaller and hasn’t spread, which makes it easier to treat successfully. The five-year relative survival rate for women with localized breast cancer (cancer that has not spread outside the breast) is nearly 99%.
A mammogram can identify changes in the breast up to two years before a patient or physician can feel them. Regular screenings can help catch the disease in its earliest stages, when it’s most treatable. This not only improves a woman’s chance of recovery but also offers more treatment options.
For example, women diagnosed with early-stage breast cancer might be candidates for breast-conserving surgery, such as lumpectomy, which involves removing the cancer and a small portion of healthy tissue around it but not the entire breast.
Moreover, early detection might also reduce the need for more aggressive treatments like chemotherapy. This can significantly lessen the physical and emotional impact of cancer treatment and improve quality of life for patients.
However, it’s essential to balance the benefits of mammograms with the potential harms, which can include false positives, over-diagnosis, and exposure to radiation. Each woman’s risk factors should be considered in decision-making about when to begin mammograms and how often to have them.
Lastly, while mammograms are a valuable tool, they are not perfect and do not detect all breast cancers. Thus, it’s crucial for women to understand and recognize any changes in their breasts and to have any changes evaluated by a healthcare professional. Awareness and early detection are key to the effective management of breast cancer.
Take Control of Your Breast Health – Schedule a Consultation with Dr. Gorman at Texas Breast Center Today
Navigating the complexities of breast cancer, its age-related risks, and the nuances of its potential causes can be challenging. That’s why Dr. Gorman and her team at Texas Breast Center are committed to offering you an advanced, personalized, and targeted approach to understanding and treating this disease. Their goal is to arm you with the knowledge you need to make informed decisions about your health and provide you with state-of-the-art care every step of the way. With a keen understanding that each patient’s journey is unique, Dr. Gorman is here to guide you through every stage of your care with empathy, expertise, and a relentless pursuit of the best outcomes possible.
Now, more than ever, it is vital for women of all ages to understand their personal risk factors for breast cancer and to engage in regular screenings. Remember, early detection is key to improving breast cancer prognosis and treatment options. We encourage you to discuss these risk factors and your personal history with a healthcare provider, like Dr. Gorman, who can help guide you through the process. Contact the Texas Breast Center today to set up an appointment for a consultation or to learn more about the services we provide. Together, we can face the challenges of breast cancer head-on and work towards a healthier, cancer-free future.
FAQ’s about Breast Cancer Causes: Age Related Risks
How much does breast cancer risk increase with age?
The risk of developing breast cancer approximately doubles every 10 years until menopause, after which the rate of increase slows. It’s estimated that around two-thirds of invasive breast cancers are found in women aged 55 or older.
Why does age increase the risk of cancer?
Age is a significant risk factor for cancer primarily due to the accumulation of genetic mutations over time and the body’s declining efficiency in repairing damaged DNA. Additionally, the immune system’s ability to detect and destroy abnormal cells decreases with age.
Why is breast cancer more common after 50?
Breast cancer is more common after 50 mainly because of the prolonged exposure to estrogen and progesterone, hormones known to stimulate cell growth in the breasts. Additionally, genetic mutations accumulate over time, increasing the likelihood of cancer development.
What is the highest age risk for breast cancer?
Breast cancer risk increases with age, with the highest incidence rates observed in women aged 70-74. However, the risk continues to be significant as women age beyond this.
Does age affect cancer survival rate?
Yes, age can affect cancer survival rates. Younger patients often have a better prognosis due to generally being healthier and better able to tolerate treatments. However, breast cancers in older women often grow more slowly and are hormone receptor-positive, which can lead to effective treatment options.
Why is breast cancer more common with age?
Breast cancer becomes more common with age due to a combination of factors such as lifetime exposure to estrogen and progesterone, the natural aging process leading to an accumulation of genetic mutations, and a decrease in the immune system’s ability to prevent the development of cancer.
Can you live 30 years after breast cancer?
Yes, it’s possible to live 30 years or more after a breast cancer diagnosis. Thanks to advancements in early detection and treatment, many women are living long, healthy lives following their diagnosis. The prognosis depends on many factors, including the cancer stage and type, the woman’s overall health, and the treatments used.
Is alcohol linked to breast cancer?
Yes, research consistently shows that drinking alcohol increases the risk of breast cancer. Even moderate consumption of an alcoholic beverage can increase breast cancer risk, and the risk increases the more alcohol is consumed.
Is breast cancer less aggressive in elderly?
Breast cancer in older women tends to be less aggressive and more responsive to hormone therapy than in younger women. This is mainly because most breast cancers in older women are hormone receptor-positive. However, diagnosis can be complicated by the presence of other age-related health conditions.
Breast cancer, a condition marked by uncontrolled cell growth in the breast tissue, continues to be one of the primary health challenges faced by women in the United States and worldwide. It is a journey that no woman should have to embark on alone, and it’s one that demands a wealth of understanding, particularly about the role of family historyin determining breast cancer risk. Recognizing this intricate tapestry of genetics and family history, Dr. Gorman and her dedicated team at Texas Breast Center provide not just treatment but holistic care that addresses each individual’s unique concerns and needs.
As we delve into the complexities of breast cancer risk, it becomes evident that this disease is a multifaceted issue, intertwining genetics, lifestyle, and environmental factors. The role of family history in determining one’s risk is particularly significant, offering insights into genetic predispositions and potential hereditary patterns. This understanding is crucial, as it guides both patients and healthcare providers in developing personalized strategies for risk assessment and management.
First-degree Relatives
First-degree blood relatives play a significant role in understanding your potential breast cancer risk. In the context of family health history, first-degree relatives refer to your father, mother, sister, brother, son, or daughter. These relationships share about 50% of their genes with you, hence why their health conditions can provide valuable insight into your own potential health risks.
Suppose a first-degree relative has been diagnosed with breast cancer. In that case, research indicates this could indicate a heightened risk of developing the disease yourself. The reasoning behind this lies in the shared genetic material between you and your first-degree relative. Certain gene mutations, such as those found in the BRCA1 or BRCA2 genes, can drastically increase the risk of breast cancer and are often passed down through generations. In addition, women with atypical hyperplasia and a first degree relative with breast cancer history have an increased risk for developing the disease.
However, a family history of breast cancer does not equate to a definitive future diagnosis. While it does raise risk levels, most cases of breast cancer are not linked to inherited gene mutations. Lifestyle factors, environmental exposures, pregnancy, and hormonal factors also significantly contribute to overall risk.
At the Texas Breast Center, we take your family history into account to provide a comprehensive risk assessment. Dr. Gorman’s approach is not only advanced but also personalized. She recognizes the importance of understanding the context of each patient’s health background, including the crucial role of first-degree relatives in determining risk. By using this information, she works with her team to develop a targeted approach, offering risk management strategies, preventive lifestyle advice, and when appropriate, genetic counseling and testing to provide a holistic health care plan.
Remember, having a close family member with breast cancer does not guarantee you will have the disease. It is one risk factor among many others, and it is important to consider it within the context of your overall health, lifestyle, and other personal risk factors. Knowing your family history is a powerful tool. It can guide you towards the necessary steps for early detection, timely medical intervention, and ultimately, it allows you to take control of your health.
Second-degree Relatives
When considering your family health history, second-degree relatives, including your grandmother, aunt, or niece, also play a critical role. These relatives share about 25% of their genetic material with you, meaning that their health conditions can still provide valuable insight into your potential health risks.
Should a second-degree relative be diagnosed with breast cancer, your risk of developing the disease may be slightly elevated. The risk associated with second-degree relatives is lower than with first-degree relatives due to the decreased proportion of shared genetic material. However, this does not make their health histories any less significant. Genetic mutations associated with breast cancer, such as those in the BRCA1 and BRCA2 genes, can still be passed along through second-degree relatives, albeit at a lower frequency.
It’s essential to remember that while the presence of breast cancer in second-degree relatives can increase your risk, most cases of breast cancer are sporadic and not due to inherited mutations. Other factors, including lifestyle, environment, and hormonal influences, can impact your breast cancer risk. Therefore, having a second-degree relative with breast cancer should be viewed as one piece of a much larger puzzle that contributes to your overall breast cancer risk.
At Texas Breast Center, we value your family’s health history as a pivotal part of your personalized breast health care journey. Dr. Gorman and her dedicated team employ a comprehensive approach, integrating the influence of both first and second-degree relatives into your overall risk assessment. By incorporating this information, we can design a targeted plan, involving advanced diagnostic screenings, preventative lifestyle recommendations, and when necessary, genetic counseling and testing.
Recognizing the importance of second-degree relatives in breast cancer risk assessment is crucial. While it doesn’t predict a certainty, it offers an opportunity for heightened vigilance, early detection, and proactive health care measures. Dr. Gorman can help you harness this knowledge, providing a platform for you to take the necessary steps to manage your health, underlining our belief that understanding and managing breast health is a collaborative, informed journey.
Multiple Family Members
When it comes to evaluating your risk of breast cancer, the significance of your family’s health history cannot be overstated. If more than one relative in your family has been diagnosed with breast cancer, it can be a key indicator of a higher risk of developing the disease. These relatives can be a combination of both first and second-degree relatives, including your mother, child, sisters, grandmothers, aunts, and nieces.
Having multiple family members with a breast cancer diagnosis can potentially suggest an inherited genetic mutation, such as in the BRCA1 or BRCA2 genes, which are associated with a substantially increased risk of breast cancer. This situation is often referred to as familial or hereditary breast cancer and it accounts for about 5-10% of all breast cancer cases. However, the presence of multiple breast cancer cases within a family may also reflect shared environmental or lifestyle factors that increase the disease’s risk.
It’s crucial to recognize that while having multiple family members with breast cancer increases your risk, it does not guarantee that you will develop the disease. The majority of breast cancer cases are actually not related to family history. Other factors, such as age, reproductive history, hormonal factors, lifestyle choices, and environmental exposures also contribute significantly to your overall risk.
The presence of multiple family members with breast cancer is an invitation for proactive health management. It offers an opportunity to heighten surveillance, encourage early detection, and equip you with the tools to manage your health effectively. At Texas Breast Center, we are your allies in this journey, offering expert advice, cutting-edge treatments, and compassionate care every step of the way.
Male Family Members
While breast cancer is predominantly associated with women, it is important to note that men can also be diagnosed with the disease. When a male family member, such as your father or brother, is diagnosed with breast cancer, it could indicate a potential inherited genetic mutation and, subsequently, an increased risk for you to develop the disease.
Male breast cancer comprises approximately 1% of all breast cancer cases, yet its significance should not be underestimated. The presence of breast cancer in a male relative such as a parent or child is often a signal of an inherited BRCA2 mutation. Although BRCA mutations increase the risk of breast cancer for both men and women, the probability of men developing breast cancer is still significantly lower compared to women. However, if a man carries a faulty BRCA gene, there is a substantial chance that he could pass it on to his children, potentially increasing their risk of developing breast cancer.
The medical diagnosis of breast cancer in a male relative underscores the importance of comprehensive family health history and genetic counseling. It’s also a stark reminder that breast cancer is not exclusive to women. However, having a male relative with breast cancer does not guarantee you will develop the disease; it merely points to a higher possibility. Multiple factors, including lifestyle choices, environmental exposures, and other genetic factors, contribute to your overall breast cancer risk.
If a male relative has been diagnosed with breast cancer, this necessitates a proactive approach to your health. Through regular screenings, potential genetic counseling and testing, and preventive lifestyle adaptations, you can help manage your risk.
Early Onset
Breast cancer is generally more common in older women, with most diagnoses made in women aged 50 and above. However, when a family member is diagnosed with breast cancer before the age of 50, it could signify an increased risk for other family members. Early-onset breast cancer often suggests a potential inherited genetic factor that can raise the risk of developing the disease.
Early-onset breast cancer, while less common, is often associated with inherited mutations in the BRCA1, BRCA2, or other related breast cancer genes. These gene mutations can be passed down from generation to generation, which could result in a higher risk of breast cancer amongst close relatives, especially if the disease occurs before the age of 50.
However, an early-onset diagnosis in the family does not confirm you will have breast cancer. It only implies a higher risk. At Texas Breast Center, we place significant importance on understanding your family’s health history. If there is a history of early-onset breast cancer in your family, this crucial information should be factored into your risk assessment and subsequently guide your breast health care management plan. This plan might include more frequent or earlier breast cancer screening, lifestyle adjustments, a healthy diet, and, where appropriate, genetic testing and counseling.
Understanding the potential implication of early-onset breast cancer in your family is a powerful tool for early detection and preventive health care. It allows for proactive risk management and heightened vigilance for any signs of the disease. At Texas Breast Center, we are here to help you navigate this journey, providing you with advanced, personalized, and compassionate care at every step of your breast health journey.
Bilateral Breast Cancer
Bilateral breast cancer, where both breasts are affected either simultaneously or sequentially, is another crucial factor when considering family history and breast cancer risk. When a family member has had cancer in both breasts, it could suggest an increased genetic susceptibility to the disease, thereby raising your own risk of developing breast cancer.
Bilateral breast cancer could indicate the presence of an inherited mutation in genes like BRCA1, BRCA2, or others related to breast cancer susceptibility. These genetic mutations can substantially raise the risk of developing breast cancer, and when observed in the context of bilateral breast cancer, can also suggest an increased likelihood of developing cancer in both breasts.
While bilateral breast cancer in a family member can be an important marker for elevated breast cancer risk, it doesn’t guarantee that you will develop the disease. The presence of bilateral breast cancer in your family history serves as a call for proactive health management. It creates an opportunity for heightened vigilance and early detection, empowering you to take the necessary steps to effectively manage your health. At Texas Breast Center, we are committed to helping you navigate this path, offering cutting-edge treatments, expert advice, and empathetic care at every stage of your journey.
Ovarian Cancer History
A family history of ovarian cancer can also increase your risk of developing breast cancer. This link is primarily due to the BRCA1 or BRCA2 gene mutations, which increase the risk of both breast and ovarian cancers. If a close relative has had ovarian cancer, consider discussing genetic testing with your healthcare provider to assess your risk.
Inherited Gene Mutations
Inherited mutations in the BRCA1 and BRCA2 genes are the most well-known genetic risk factors for breast cancer. These mutations can significantly increase your risk for breast cancer. Other gene mutations associated with breast cancer include p53, PTEN, and CHEK2. Genetic counseling and testing can provide information about these inherited risks and guide risk management strategies.
Other Related Cancers
Breast cancer risk is not solely influenced by a family history of breast cancer itself. Other related cancers, such as prostate cancer, pancreatic cancer, or other types of cancer, in your family can also be indicative of an increased risk of developing breast cancer. This suggests that certain inherited genetic mutations may not only predispose individuals to breast cancer but also to other forms of malignancies.
For instance, a BRCA mutation, while primarily associated with breast and ovarian cancer, has also been linked to a higher risk of prostate and pancreatic cancers. Similarly, mutations in other genes, such as PALB2, can increase the risk of both breast and pancreatic cancers. Therefore, a family history of these other cancers can provide vital clues about your potential inherited risk of developing breast cancer.
However, the presence of other related cancers in your family doesn’t necessarily mean you will develop breast cancer. It’s a single piece of the puzzle in the larger landscape of breast cancer risk. Your overall risk is influenced by a complex interplay of genetic, hormonal, environmental, and lifestyle factors.
At Texas Breast Center, we recognize the importance of a comprehensive family cancer history in understanding your unique breast cancer risk profile. Dr. Gorman, known for her commitment to providing advanced, personalized, and targeted breast cancer care, considers the entire scope of your family’s cancer history during risk assessment. This thorough evaluation can inform your personalized risk management strategy, including regular screening schedules, lifestyle modifications, and potentially genetic counseling and testing.
A family history of related cancers calls for an informed, proactive approach to your breast health. It’s an opportunity for attentive monitoring, early detection, and more effective risk management. At Texas Breast Center, we are here to support and guide you every step of the way, offering expert medical advice, leading-edge treatments, and compassionate care tailored to your unique needs.
Ethnic Background
Certain ethnic backgrounds, such as Ashkenazi Jews, are associated with a higher prevalence of BRCA1 and BRCA2 mutations, thus leading to an increased risk of breast cancer. Understanding your family’s ethnic background can help clarify your risk and inform screening recommendations.
Understanding these familial and genetic factors is critical in guiding breast cancer risk assessment and management strategies. However, keep in mind that having one or even multiple breast cancer risk factors does not guarantee a breast cancer diagnosis. Many women with one or more risk factors never develop the disease, and some women with breast cancer have no known risk factors other than being a woman and growing older.
In conclusion, a family history of breast cancer can significantly influence an individual’s risk of developing the disease. However, it’s important to remember that breast cancer is not exclusively hereditary. Environmental factors, lifestyle choices, and certain conditions such as obesity, high alcohol intake, lack of breastfeeding, early menstruation, late menopause, and exposure to hormone replacement therapy can contribute to breast cancer risk.
Dense breast tissue, characterized by a higher proportion of glandular and connective tissue to fatty or adipose tissue, can also increase the risk and make mammography screening more challenging. Factors such as age, hormone levels, and certain drugs can affect breast density.
Knowledge and awareness of both your familial and personal risk factors can empower you to take control of your breast health. Regular screenings, maintaining a healthy body weight, limiting alcohol intake, and understanding the implications of your birth control choices are ways to manage and reduce your risk.
If you have a family history of breast cancer or other related cancers, consider speaking with a healthcare provider or a genetic counselor. They can provide you with valuable information, discuss the possibility of genetic testing, and guide you towards the best preventative measures and screenings based on your risk.
At Texas Breast Center, we recognize that every patient is unique, and we are committed to providing advanced, personalized, and targeted care. Dr. Gorman and her dedicated team strive to empower patients with the knowledge and resources necessary to make informed decisions about their health. If you have concerns about your breast cancer risk, contact the Texas Breast Center to schedule an appointment.
In the realm of breast health, understanding your risk is the first step towards prevention and early detection. Through shared decision-making and a patient-centered approach, we can work together to navigate your breast cancer risk and ensure that you receive the most appropriate, tailored care.
Remember, knowledge is power. Take control of your health today.
See the other articles in the Causes series, including Age-Related Risks.
Texas Breast Center – Helping You 0n Your Journey
Our philosophy is rooted in a strong dedication to advanced, personalized, and targeted breast cancer care. We believe that every woman is more than just a patient – she is a person with a unique story and a unique health journey. Our mission is to walk with you, hand-in-hand, through each step of this journey, offering the most advanced treatments, answering your every question, and standing as a constant source of support and knowledge.
Moreover, we understand that breast cancer risk is not just a clinical concept—it’s an intimate part of a woman’s life, shaping her decisions and future. This understanding is our driving force. Through fostering a supportive environment and leveraging advanced targeted treatment strategies, we provide personalized care to every woman walking through our doors. Our comprehensive approach ensures that your journey toward understanding, managing, and potentially preventing breast cancer is one of empowerment, care, and expert support.
At Texas Breast Center, we blend our advanced medical expertise with warmth, understanding, and the unwavering belief that knowledge is indeed power. Join us as we delve deeper into the role of family history in influencing breast cancer risk. Our goal is to empower you to take proactive steps toward safeguarding your health and share important information to help prevent breast cancer. Your journey is our journey, and we’re here with you every step of the way.
A breast cancer diagnosis can bring about an overwhelming amount of decisions to be made. First and foremost on most patients’ minds is what are the treatment options and which have the best long-term outcomes. Choosing a doctor that you feel comfortable having open and honest communication with will help alleviate some of the stress associated with making treatment decisions.
Dr. Gorman is committed to giving her breast cancer patients an advanced, personalized, and targeted approach to breast cancer treatments. In some cases, people with breast cancer can choose between removing the entire breast (mastectomy) or breast-conserving surgery (lumpectomy) followed by radiation. In this article, we will discuss the differences in long-term outcomes between lumpectomy and mastectomy procedures when performed by a skilled surgeon.
What is a mastectomy?
Breast surgery that involves the removal of the entire breast is called a mastectomy. When faced with the choice between a mastectomy and lumpectomy (also known as breast-conserving surgery) plus radiation therapy, some women choose mastectomy. For some women, mastectomy is the only surgery option for breast cancer. Mastectomy is also used to treat breast cancer that has come back after lumpectomy and radiation therapy have been done.
Total (simple) mastectomy and modified radical mastectomy are the two main types of mastectomy. Your diagnosis and cancer type will determine the type of mastectomy you will have.
Total (Simple) Mastectomy
In a total (simple) mastectomy, the surgeon removes the entire breast and the lining of the chest muscle but does not take out any other tissue.
Total (simple) mastectomy can be used to treat:
Ductal carcinoma in situ (DCIS)
Paget disease of the breast with underlying DCIS
Invasive breast cancer
Breast cancer recurrence
Total mastectomy is also performed on high-risk women who want to prevent cancer based on personal preferences.
Sometimes a reconstruction of the breast is done at the same time as a mastectomy.
Modified radical mastectomy
The breast surgeon takes out the entire breast, the lining of the chest muscles, and the lymph nodes in the armpit area (axillary lymph nodes) during a modified radical mastectomy.
This type of surgery can be used to treat:
Invasive breast cancer
Inflammatory breast cancer
Paget disease of the breast with underlying invasive breast cancer
Sometimes a modified radical mastectomy is done at the same time as breast reconstruction. However, this is not done for inflammatory breast cancer.
What is a lumpectomy?
A lumpectomy is a surgical procedure used to remove breast cancer. In contrast to a mastectomy, a lumpectomy only removes the breast tumor and a small amount of healthy tissue around it. It leaves most of the skin and breast tissues where they are.
The breast looks as close as possible to how it did before surgery after a lumpectomy. Most of the time, the breast and nipple area keep their general shape. Lumpectomy is also called breast conserving surgery, partial mastectomy, and wide excision. This type of breast cancer treatment is used in early breast cancer.
Is there a difference in the long-term outcomes of a mastectomy vs. a lumpectomy?
For women with earlystage breast cancer, there is no difference in overall survival rates between a mastectomy and a lumpectomy with radiation. There are other differences between these two therapies, but neither is better than the other. It just depends on what’s best for the patient.
There have been multiple randomized trials comparing breast-conserving surgery and mastectomy, which found no survival advantage for either surgery option. In 1990, the American National Cancer Institute (NCI) consensus panel came to the conclusion that breast-conserving surgery was the optimal treatment based on these trials in the United States. Since then, the trend in surgical procedures has changed, with breast-conserving surgery first increasing and then dropping since 2006 while mastectomy rates have climbed. Bilateral mastectomies are primarily responsible for the rise in mastectomy rates.
Studies show that women with early-stage breast cancer who have breast-conserving surgery followed by radiation therapy have the same chance of surviving as women who have a mastectomy. This means that if there is no medical reason for you to have one surgery over the other, your doctor will let you choose.
Choosing between surgery to save the breasts and a mastectomy is a very personal decision. In addition, it comes at a very emotional time. Your feelings, preferences, priorities, and way of life all affect your choice. If you want to keep as much of your breast as possible, you might choose breast conserving therapy. Or, a mastectomy, which removes more breast tissue, may give you more peace of mind.
First, talk to your breast physician to find out if you can choose between a mastectomy and a lumpectomy plus radiation therapy. Some women may not have a choice because a mastectomy is the only surgery that can treat their advanced breast cancer. About 25% of women will need a mastectomy, but the other 75% can choose not to have one.
Most of the time, the size of the tumor compared to the size of the breast is the main thing a breast surgeon looks at to decide if a lumpectomy is a good option for the treatment of cancer. Whether lumpectomy is a realistic possibility is related to the % volume of the breast which requires excision to remove the cancer with adequate pathological margins, in comparison to the overall size of the breast, also taking into account where the tumor lies within the breast, as some areas of the breast are more cosmetically sensitive to volume loss than others.
Chemotherapy or hormone therapy may be suggested before surgery, especially if you have a large tumor or if your lymphatic system is involved. This is called neoadjuvant therapy, and it will help shrink the tumor before surgery to remove breast cancer.
Sometimes a woman can have a lumpectomy but should avoid radiation therapy, and in this case, she will need to have a mastectomy instead. Radiation therapy is not for everyone. Radiation therapy can be dangerous if you are pregnant or if you have certain health problems.
Since radiation can hurt the baby, it is not given to women who are pregnant. Depending on when the woman found out she was pregnant and when she was told she had breast cancer, she may be able to have a lumpectomy and put off radiation therapy until after she gives birth.
Some serious diseases of the connective tissues, like scleroderma or lupus, may make you more sensitive to the side effects of radiation therapy. However, in some women at higher risk of breast cancer recurrence, radiation therapy may still be used.
Radiation therapy to the same breast or the same side of the chest in the past may make you ineligible for radiation therapy if there is a recurrence. In most cases, breast radiation therapy can only be done once. After careful discussion with your radiation oncologist, radiation therapy may be given to the same breast again in very rare cases.
If you have a choice, you should carefully consider all of the outcomes before making a decision. A short delay before surgery won’t hurt your prognosis. Think about the risks and benefits of each surgery and choose the one that is best for you. No matter which choice you make, the chance of survival is the same.
How do patients choose between a mastectomy versus lumpectomy plus radiation therapy?
People with breast cancer can sometimes choose between the total removal of a breast (mastectomy) and surgery to save the breast (lumpectomy) followed by radiation. If there is only one site of cancer in the breast and the tumor is less than 4 centimeters, a lumpectomy followed by radiation is commonly a treatment option and is likely to work just as well as a mastectomy. Clear margins (no cancer cells in the tissue surrounding the tumor) are also a requirement for a lumpectomy.
When given the option, most women choose the less invasive lumpectomy, but there are a few things to consider before making the decision between lumpectomy and mastectomy. Consider how you feel about these factors:
How important to you is it to keep your breast? If keeping your breast is important to you, you might choose to have a lumpectomy with radiation instead of a mastectomy and avoid having the entire breast removed.
Do you want your breasts to be as close to the same size as possible? Most women look good cosmetically after having a lumpectomy. When a larger area of tissue needs to be removed, which happens very rarely, a lumpectomy can make the breast look smaller or distorted. There are different types of reconstruction for both lumpectomy (if there is a lot of distortion) and mastectomy. It is up to you and your health care provider to determine the best course of action if you require a significant amount of tissue removed and want breasts that are the same size.
How concerned are you about a recurrence of breast cancer? If removing the entire breast would make you less worried about your chances of recurrence, you might want to get a mastectomy.
Ultimately the decision to have a lumpectomy plus radiation therapy or a mastectomy is a very personal decision that should be made with the guidance of your skilled surgeon. Dr. Gorman at Texas Breast Center is a breast surgeon who specializes in surgical oncology and surgical diseases of the breast. She treats each patient as an individual and tailors their treatment plan to their unique needs knowing that no two people are the same and, therefore, treatment cannot be either.
Dr. Gorman has a vast amount of knowledge and experience when it comes to the treatment for breast cancer. She always considers and evaluates all of the treatment options and their likelihood of success before contemplating surgery. When surgery is needed, she implements a breast-conserving surgery when possible to reduce the impact on cosmetic appearance post-operation. For more information about Dr. Gorman and the breast cancer surgery treatments available at Texas Breast Center, visit our website or call our office to schedule a consultation.
Breast cancer is the most common among cancers in women worldwide, with an estimated 2.3 million new cases diagnosed in 2020 alone. While there are many factors that can contribute to the development of breast cancer, one of the most important is genetics. Certain genetic mutations can significantly increase a person’s risk of developing Breast cancer is the most common cancer in women around the world, with about 2.3 million new cases expected to be found in 2020 alone. Even though there are many things that can lead to breast cancer, genes are one of the most important ones. Some changes in a person’s genes can make it much more likely that they will get breast cancer or another type of cancer. In this article, we will explore the most common genetic mutations associated with breast cancer risk, how they are inherited, and what can be done to manage that risk.
BRCA1 and BRCA2 Mutations
BRCA1 and BRCA2 are two of the most well-known genetic mutations associated with breast cancer risk. These genes produce proteins that help to suppress tumor growth, but mutations in these genes can disrupt this function and increase the risk of developing breast and ovarian cancer.
Breast cancer genes, such as BRCA1 and BRCA2, have been identified as major risk factors for invasive breast cancer. These genes are involved in regulating cell growth and repair, and when mutated, they can disrupt normal cellular processes in breast tissue. Mutations in these breast cancer genes can be inherited or acquired, and women with a family history of breast cancer are at higher risk. Other breast cancer risk factors include age, gender, lifestyle factors, and exposure to certain chemicals. Early detection through regular mammograms and other breast cancer screening methods is critical for improving outcomes for women with invasive breast cancer. As research continues to uncover new insights into the biology of breast cancer, identifying and understanding these risk factors will be critical for reducing the burden of this disease on women worldwide.
What is the definition and function of BRCA1 and BRCA2?
BRCA1 and BRCA2 are tumor suppressor genes, which means they produce proteins that help to regulate cell growth and division. Specifically, these proteins help to repair damaged DNA and prevent cells from growing and dividing too rapidly or uncontrollably. Mutations in these genes can interfere with the production of these proteins, leading to a higher risk of developing cancer.
What are the inheritance patterns of BRCA1 and BRCA2?
BRCA1 and BRCA2 mutations are inherited in an autosomal dominant pattern. This means that a person only needs to inherit a mutated copy of the gene from one parent to be at risk of developing cancer. A child of a parent with a BRCA1 or BRCA2 mutation has a 50% chance of inheriting the mutation.
Is there an increased risk of breast and ovarian cancer with BRCA1 and BRCA2 mutations?
Women with a BRCA1 or BRCA2 mutation have a significantly increased risk of developing breast and ovarian cancer. According to the National Cancer Institute, women with a BRCA1 or BRCA2 mutation have a:
55-72% chance of developing breast cancer by age 70 (compared to 12% in the general population)
44% chance of developing ovarian cancer by age 80 (compared to 1.3% in the general population)
Other cancers may also be associated with BRCA mutations, including prostate cancer in men.
What are screening and prevention options for people with BRCA1 and BRCA2 mutations?
Due to the increased risk of breast and ovarian cancer associated with BRCA mutations, women who carry a BRCA1 or BRCA2 mutation are typically advised to undergo increased surveillance and risk reduction measures.
Surveillance may involve more frequent mammograms and breast MRIs, as well as screening for ovarian cancer using blood tests and/or ultrasounds. In some cases, prophylactic surgery (such as mastectomy or oophorectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for BRCA1 and BRCA2 mutations?
Genetic testing is available to determine whether someone has a BRCA1 or BRCA2 mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the genes. It is important to note that not everyone who is at risk of carrying a BRCA mutation will have one, and not everyone who has a BRCA mutation will develop cancer.
Genetic counseling and testing are typically recommended for people with a family history of breast or ovarian cancer, especially if multiple family members have been diagnosed with the disease at a young age. Genetic counseling is also recommended before and after testing to help individuals understand their risk, the implications of testing, and the options available for managing that risk.
While BRCA1 and BRCA2 are the most well-known genetic mutations associated with breast cancer risk, there are many other mutations that can also increase a person’s risk of developing the disease.
PALB2 Mutations
PALB2 (Partner and Localizer of BRCA2) is a gene that produces a protein that interacts with the BRCA2 protein to help repair damaged DNA. Mutations in PALB2 can increase the risk of developing breast cancer and may also increase the risk of pancreatic cancer.
What is the definition and function of PALB2?
PALB2 is a tumor suppressor gene that plays a role in repairing damaged DNA. It produces a protein that interacts with the BRCA2 protein to help repair double-stranded DNA breaks. Mutations in PALB2 can interfere with this function and increase the risk of developing breast cancer.
What are the inheritance patterns of PALB2?
PALB2 mutations are inherited in an autosomal recessive pattern. This means that a person must inherit two copies of the mutated gene (one from each parent) to be at risk of developing cancer. A child of two carriers of a PALB2 mutation has a 25% chance of inheriting the mutation.
Is there an increased risk of breast and ovarian cancer for people with a PALB2 mutation?
Women with a PALB2 mutation have a slightly increased risk of developing breast cancer. According to the National Cancer Institute, women with a PALB2 mutation have:
33% chance of developing breast cancer by age 70 (compared to 12% in the general population)
What are screening and prevention options for people with a PALB2 mutation?
Surveillance may involve more frequent mammograms and breast MRIs. In some cases, prophylactic surgery (such as mastectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for a PALB2 mutation?
Genetic testing is available to determine whether someone has a PALB2 mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the gene. It is important to note that not everyone who is at risk of carrying a PALB2 mutation will have one, and not everyone who has a PALB2 mutation will develop cancer.
TP53 Mutations
TP53 is a gene that produces a protein called p53, which helps to regulate cell growth and prevent the development of tumors. Mutations in TP53 can interfere with the function of p53 and increase the risk of developing various types of cancer, including breast cancer.
What is the definition and function of TP53?
TP53 is a tumor suppressor gene that produces a protein called p53. This protein helps to regulate cell growth and prevent the development of tumors by responding to DNA damage and other cellular stresses. Mutations in TP53 can interfere with the function of p53, leading to a higher risk of developing cancer.
What are the inheritance patterns of TP53?
TP53 mutations are inherited in an autosomal dominant pattern. A child of a parent with a TP53 mutation has a 50% chance of inheriting the mutation.
Is there an increased risk of breast cancer for people with a TP53 mutation?
Women with a TP53 mutation have an increased risk of developing various types of cancer, including breast cancer. According to the National Cancer Institute, women with a TP53 mutation have:
49% chance of developing breast cancer by age 70 (compared to 12% in the general population)
Increased risk of other cancers, including brain, bone, and soft tissue tumors
What are screening and prevention options for people with a TP53 mutation?
Surveillance may involve more frequent mammograms and breast MRIs, as well as screening for other types of cancer. In some cases, prophylactic surgery (such as mastectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for a TP53 mutation?
Genetic testing is available to determine whether someone has a TP53 mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the gene. It is important to note that not everyone who is at risk of carrying a TP53 mutation will have one, and not everyone who has a TP53 mutation will develop cancer.
CHEK2 Mutations
CHEK2 is a gene that produces a protein called checkpoint kinase 2, which helps to regulate cell growth and division. Mutations in CHEK2 can interfere with this function and increase the risk of developing breast cancer.
What is the definition and function of CHEK2?
CHEK2 is a checkpoint kinase that helps to regulate cell growth and division. It produces a protein that responds to DNA damage and other cellular stresses to prevent the development of tumors. Mutations in CHEK2 can interfere with the function of this protein, leading to a higher risk of developing cancer.
What are the inheritance patterns of CHEK2?
CHEK2 mutations are inherited in an autosomal dominant pattern. A child of a parent with a CHEK2 mutation has a 50% chance of inheriting the mutation.
Is there an increased risk of breast cancer for people with a CHEK2 mutation?
Women with a CHEK2 mutation have a moderately increased risk of developing breast cancer. According to the National Cancer Institute, women with a CHEK2 mutation have a:
20-30% chance of developing breast cancer by age 80 (compared to 12% in the general population)
What are screening and prevention options for people with a CHEK2 mutation?
Surveillance may involve more frequent mammograms and breast MRIs. In some cases, prophylactic surgery (such as mastectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for a CHEK2 mutation?
Genetic testing is available to determine whether someone has a CHEK2 mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the gene. It is important to note that not everyone who is at risk of carrying a CHEK2 mutation will have one, and not everyone who has a CHEK2 mutation will develop cancer.
ATM Mutations
ATM is a gene that produces a protein called ataxia-telangiectasia mutated, which helps to regulate cell growth and division. Mutations in ATM can interfere with this function and increase the risk of developing breast cancer.
What is the definition and function of ATM?
ATM is a protein kinase that helps to regulate cell growth and division. It produces a protein that responds to DNA damage and other cellular stresses to prevent the development of tumors. Mutations in ATM can interfere with the function of this protein, leading to a higher risk of developing cancer.
What are the inheritance patterns of ATM?
ATM mutations are inherited in an autosomal dominant pattern. A child of a parent with an ATM mutation has a 50% chance of inheriting the mutation.
Is there an increased risk of breast cancer for people with an ATM mutation?
Women with an ATM mutation have a moderately increased risk of developing breast cancer. According to the National Cancer Institute, women with an ATM mutation have a:
14-29% chance of developing breast cancer by age 70 (compared to 12% in the general population)
What are screening and prevention options for people with an ATM mutation?
Surveillance may involve more frequent mammograms and breast MRIs. In some cases, prophylactic surgery (such as mastectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for an ATM mutation?
Genetic testing is available to determine whether someone has an ATM mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the gene. It is important to note that not everyone who is at risk of carrying an ATM mutation will have one, and not everyone who has an ATM mutation will develop cancer.
PTEN Mutations
PTEN is a gene that produces a protein called phosphatase and tensin homolog, which helps to regulate cell growth and division. Mutations in PTEN can interfere with this function and increase the risk of developing breast, thyroid, and other types of cancer.
What is the definition and function of PTEN?
PTEN is a tumor suppressor gene that produces a protein called phosphatase and tensin homolog. This protein helps to regulate cell growth and division by suppressing a signaling pathway that promotes cell growth. Mutations in PTEN can interfere with the function of this protein, leading to a higher risk of developing cancer.
What are the inheritance patterns of PTEN?
PTEN mutations are inherited in an autosomal dominant pattern. A child of a parent with a PTEN mutation has a 50% chance of inheriting the mutation.
Is there an increased risk of breast, thyroid, and other cancers for people with a PTEN mutation?
People with a PTEN mutation have an increased risk of developing various types of cancer, including breast and thyroid cancer. According to the National Cancer Institute, people with a PTEN mutation have a:
85% chance of developing breast cancer by age 70 (compared to 12% in the general population)
Increased risk of other cancers, including thyroid and endometrial cancer
What are screening and prevention options for people with a PTEN mutation?
Surveillance may involve more frequent mammograms and breast MRIs, as well as screening for thyroid and other types of cancer. In some cases, prophylactic surgery (such as mastectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for a PTEN mutation?
Genetic testing is available to determine whether someone has a PTEN mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the gene. It is important to note that not everyone who is at risk of carrying a PTEN mutation will have one, and not everyone who has a PTEN mutation will develop cancer.
CDH1 Mutations
CDH1 is a gene that produces a protein called cadherin-1, which helps to maintain the structure of cells in tissues such as the breast and stomach. Mutations in CDH1 can interfere with this function and increase the risk of developing hereditary diffuse gastric cancer syndrome and breast cancer.
What is the definition and function of CDH1?
CDH1 is a gene that produces a protein called cadherin-1. This protein helps to maintain the structure of cells in tissues such as the breast and stomach by allowing cells to stick together. Mutations in CDH1 can interfere with the function of this protein, leading to a higher risk of developing hereditary diffuse gastric cancer syndrome and breast cancer.
What are the inheritance patterns of CDH1?
CDH1 mutations are inherited in an autosomal dominant pattern. A child of a parent with a CDH1 mutation has a 50% chance of inheriting the mutation.
Is there an increased risk of hereditary diffuse gastric cancer syndrome and breast cancers for people with a CDH1 mutation?
People with a CDH1 mutation have an increased risk of developing hereditary diffuse gastric cancer syndrome, which is a rare type of stomach cancer. They also have an increased risk of developing lobular breast cancer, which is a type of breast cancer that begins in the milk-producing glands.
What are screening and prevention options for people with a CDH1 mutation?
Surveillance may involve regular endoscopies to screen for stomach cancer, as well as more frequent mammograms and breast MRIs, to screen for breast cancer. In some cases, prophylactic surgery (such as mastectomy or gastrectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for a CDH1 mutation?
Genetic testing is available to determine whether someone has a CDH1 mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the gene. It is important to note that not everyone who is at risk of carrying a CDH1 mutation will have one, and not everyone who has a CDH1 mutation will develop cancer.
STK11 Mutations
STK11 is a gene that produces a protein called serine/threonine kinase 11, which helps to regulate cell growth and division. Mutations in STK11 can interfere with this function and increase the risk of developing Peutz-Jeghers syndrome and breast cancer.
What is the definition and function of STK11?
STK11 is a serine/threonine kinase that helps to regulate cell growth and division. It produces a protein that responds to cellular stresses to prevent the development of tumors. Mutations in STK11 can interfere with the function of this protein, leading to a higher risk of developing cancer.
What are the inheritance patterns of STK11?
STK11 mutations are inherited in an autosomal dominant pattern. A child of a parent with an STK11 mutation has a 50% chance of inheriting the mutation.
Is there an increased risk of Peutz-Jeghers Syndrome and Breast Cancer for people with a STK11 mutation?
People with an STK11 mutation have an increased risk of developing Peutz-Jeghers syndrome, which is a rare genetic disorder characterized by the development of benign growths in the digestive tract and an increased risk of developing certain types of cancer. They also have an increased risk of developing breast cancer.
What are screening and prevention options for people with an STK11 mutation?
Surveillance may involve regular colonoscopies to screen for polyps and other growths in the digestive tract, as well as more frequent mammograms and breast MRIs to screen for breast cancer. In some cases, prophylactic surgery (such as mastectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for an STK11 mutation?
Genetic testing for breast cancer is available to determine whether someone has an STK11 mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the gene. It is important to note that not everyone who is at risk of carrying an STK11 mutation will have one, and not everyone who has an STK11 mutation will develop cancer.
NF1 Mutations
NF1 is a gene that produces a protein called neurofibromin 1, which helps to regulate cell growth and division. Mutations in NF1 can interfere with this function and increase the risk of developing neurofibromatosis type 1 and breast cancer.
What is the definition and function of NF1?
NF1 is a gene that produces a protein called neurofibromin 1. This protein helps to regulate cell growth and division by suppressing a signaling pathway that promotes cell growth. Mutations in NF1 can interfere with the function of this protein, leading to a higher risk of developing neurofibromatosis type 1 and breast cancer.
What are the inheritance patterns of NF1?
NF1 mutations are inherited in an autosomal dominant pattern. A child of a parent with an NF1 mutation has a 50% chance of inheriting the mutation.
Is there an increased risk of Neurofibromatosis Type 1 and Breast Cancer for people with an NF1 mutation?
People with an NF1 mutation have an increased risk of developing neurofibromatosis type 1, which is a rare genetic disorder characterized by the development of benign growths in the nervous system and other parts of the body. They also have an increased risk of developing breast cancer.
What are screening and prevention options for people with an NF1 mutation?
Surveillance may involve regular MRIs to screen for growths in the nervous system and other parts of the body, as well as more frequent mammograms and breast MRIs to screen for breast cancer. In some cases, prophylactic surgery (such as mastectomy) may be recommended to reduce the risk of developing cancer.
Is there genetic testing for an NF1 mutation?
There are genetic tests available to determine whether someone has an NF1 mutation. The test involves analyzing a sample of blood or saliva to look for changes or abnormalities in the gene. It is important to note that not everyone who is at risk of carrying an NF1 mutation will have one, and not everyone who has an NF1 mutation will develop cancer.
Conclusion
Genetic mutations play an important role in the development of breast cancer. In some cases, gene mutations can be inherited and increase the likelihood that an individual will develop breast cancer over their lifetime. Those who have a family history of breast cancer or who have other risk factors should consider genetic testing to determine whether they carry a mutation that increases their risk of developing hereditary breast cancer. By identifying these mutations, patients can take steps to reduce their risk of developing breast cancer through increased surveillance, prophylactic surgery, and other interventions.
At Texas Breast Center, we offer advanced, personalized, and targeted approaches to breast cancer care, including genetic testing and counseling, to help our patients make informed decisions about their health. Our team of expert breast surgeons, oncologists, and other healthcare professionals is dedicated to providing comprehensive care and support throughout every stage of the breast cancer journey. We understand that a breast cancer diagnosis can be overwhelming, and we are here to help guide our patients through the process with compassion, expertise, and a focus on personalized care.
If you have questions about genetic mutations and breast cancer or are interested in learning more information about our breast cancer services, please don’t hesitate to contact Texas Breast Center to schedule a consultation. We are committed to helping our patients achieve the best possible outcomes and live their lives to the fullest.
At Texas Breast Center, Dr. Gorman is dedicated to offering breast cancer patients the most cutting-edge, individualized, and targeted breast surgery and breast cancer treatments available. Because of this, she partners with other doctors to offer her patients a team approach to their treatment and recovery. She expertly guides patients through the process of determining the most appropriate cancer treatment options and the most beneficial surgical procedures. But, she is aware that she is not the final stage of the healing journey. Reconstruction after mastectomy for breast cancer is a common medical necessity. As a result, Dr. Gorman has partnered with Dr. Potter to offer breast reconstruction to her patients for more than 15 years.
Dr. Gorman always has her patients in mind and strives to keep them informed of any changes or developments that could potentially affect them during their course of treatment. Recently there has been a change in insurance coding that could affect patients planning to have the DIEP flap method of breast reconstruction, which she would like to make patients aware of.
What is DIEP flap surgery?
DIEP flap surgery is a method of breast reconstruction. DIEP stands for the deep inferior epigastric perforator artery, which runs through the abdomen. DIEP flap surgery involves transferring fat, skin, and blood vessels from the abdominal wall to the chest in order to reconstruct the breast. A DIEP flap is regarded as a muscle-sparing type of flap.
Using microsurgery, the surgeon reconnects the flap’s blood vessels to the patient’s existing blood vessels in the chest. Because no muscle is harvested for the DIEP flap, most women have a shorter recovery time and a reduced chance of losing abdominal muscular strength compared to the TRAM flap procedures.
Not every surgeon is qualified to do DIEP flaps, and the technique is not offered at all hospitals because it necessitates specialized training and knowledge in microsurgery. This is why it is important to find a skilled reconstructive surgeon like Dr. Potter, who has been performing these procedures for over 15 years.
Will health insurance companies cover DIEP flap surgery?
In spite of the fact that the DIEP flap surgery has been covered by the vast majority of commercial health insurance providers since 2007, doctors may soon be unable to bill insurance companies because the procedure will no longer have a unique billing code.
The Centers for Medicare & Medicaid Services (CMS) is a federal agency responsible for enforcing the use of specific billing codes for medical services. These codes are used by doctors to charge a medical insurance company, which may cover all or part of the amount, depending on the policy. There used to be separate ICD-10 codes for DIEP flap breast reconstruction and other perforator flap breast reconstruction surgeries.
The decision to group all breast reconstruction surgeries using flaps under a single code was made by CMS in 2019, and the agency plans to completely phase out the use of individual procedure-specific codes by the end of 2024. As a result, insurance companies will only pay what they would have paid for TRAM flap surgery, an older, less sophisticated, and less common treatment of cancer that is linked to more long-term risks than when a surgeon performs DIEP flap surgery. It’s estimated that the cost of TRAM flap surgery is between 70 and 90 percent less than that of DIEP flap surgery.
At that rate, health care professionals simply cannot afford to offer DIEP flap surgery, so patients are left with two options: pay out of pocket for the procedure (which can cost over $50,000) or settle with less ideal treatment options.
Some health insurance issuers have already stopped covering DIEP flap surgery even before the coding changes take effect next year. Some doctors are now declining to do the procedure altogether even if the patient’s insurance policy still covers it, while others will only do so if their patients can pay the full cost of the operation upfront.
All commercial health insurance policies may discontinue covering DIEP flap surgery between now and next year if CMS’s decision is not reversed soon.
What about the Women’s Health and Cancer Rights Act of 1998 (WHCRA) and the Affordable Care Act?
United States federal law and some state laws guarantee that women can use their health insurance plan to pay for breast reconstruction if they need it. Group health plans and health insurance companies (including HMOs) are obligated to cover all phases of medical care, including breast reconstruction, if they pay for a mastectomy under the Women’s Health and Cancer Rights Act of 1998 (WHCRA). While the law does provide mandatory coverage for mastectomy and breast reconstruction, the regulation does not outline the specific procedures of breast reconstruction that must be covered, making this coding change problematic.
The WHCRA does not apply to some types of health insurance programs, including some self-funded, short-term, government health plans and plans sponsored by religious organizations. Medical assistance programs like Medicare and Medicaid are likewise excluded from the restrictions of the law. They operate by their own set of standards. Medicare covers breast reconstruction using breast prostheses if you had a mastectomy because of breast cancer. Medicaid coverage for breast reconstruction varies by state.
Under the Affordable Care Act, health insurance companies must cover breast cancer treatment and follow-up care. But again, it does not guarantee which specific procedure must be covered.
What can patients do?
Get in touch with your senator and local representative and ask them to lobby CMS to reverse the changes made to the descriptor of CPT code 19364 and restore billing codes S2068 (for DIEP flap surgery), S2066 (for SGAP surgery), and S2067 (for stacked flap surgery). Doing so helps guarantee that all forms of breast reconstruction will be covered by health insurance plans for women who have been diagnosed with breast cancer.
If you have had or are considering DIEP flap reconstruction, you may want to write about your experience and explain the significance of the procedure to you and your breast cancer therapy and how important health insurance coverage is for this surgery.
There are some financial assistance programs for women facing breast cancer that are available for breast cancer treatment that may be able to help with the medical expenses of breast reconstruction if it is not covered by your individual health policy.
A breast cancer diagnosis can be a stressful time, and Dr. Gorman makes it her mission to ease the burden through an advanced, personalized, and targeted approach to treatment. For more information about breast cancer treatment, breast cancer surgery options, and the compassionate care offered by Dr. Gorman at Texas Breast Center, visit the website or call to schedule your consultation.
Several forms of breast cancer are more likely to develop as people age. However, improvements in diagnosis and highly customized treatment regimens are raising the likelihood of recovery for elderly women and enabling many to lead longer, healthier lives despite developing breast cancer. There are several treatment choices for older adults with breast cancer that have positive outcomes, depending on the patient’s health and personal preferences.
What are the common types of breast cancer diagnosed in older patients?
Invasive ductal carcinoma, also known as IDC, and invasive lobular carcinoma, also known as ILC, are the two types of breast cancers in women most frequently diagnosed in this age group. Although they develop in different breast tissues, these tumors are treated similarly.
Hormone receptor positive tumors make up the majority of invasive malignancies in this age range. Breast cancers in elderly patients that are hormone-positive tend to grow slowly, which is hopeful news for patients and can mean a good prognosis and successful breast cancer management.
How does a patient’s age impact treatment decisions?
There is no reason to put off treating breast cancer in an older adult if she is otherwise healthy.
A patient’s treatment options become more challenging if she is ill, particularly if she has a condition like dementia or Parkinson’s disease. While these factors make treatment more complicated, oncologists can still treat patients to increase comfort, even in these circumstances.
A patient’s functional age should be taken into account more so than their chronological age when making decisions about breast cancer treatment and breast cancer care. The functional age factors in the patient’s physical limits, comorbidities, and social support. For patients with breast cancer who are older but physically strong and otherwise healthy, all treatment options available to younger patients should be considered, including surgery if the patient has operable breast cancer. Chemotherapy, trastuzumab, and radiotherapy should be provided as routine adjuvant therapy to women with breast cancer who are older than 65 and whose life expectancy is greater than five years, and who are otherwise in good health. In patients who are frail, adjuvant therapies might be scaled back or abandoned. Enrollment in clinical trials should also be available to patients over the age of 65.
More FAQ’s about Treating Breast Cancer in Older Adults
What breast cancer treatment is most effective for elderly patients?
Doctors consider the features of the tumor when determining which treatment plan could be appropriate for a certain patient. This can help distinguish between tumors that may respond to other forms of treatment and those that are likely to respond to hormone-blocking therapy alone.
Mapping the genome of cancer cells through genomic breast cancer testing (also known as Oncotype tests) can help determine whether or not they will respond to hormone-blocking therapy, chemotherapy, or both. While Oncotype tests are not recommended for all patients, some with invasive tumors larger than 0.5 cm and estrogen-positive, the tests can reveal whether a particular breast cancer recurrence is likely following treatment.
Genetic testing for breast cancer in the elderly can now provide information on more advanced breast tumors, including those that have invaded the lymph nodes. With the aid of these findings, your doctor is better equipped than ever to suggest a treatment strategy for controlling breast cancer.
Do larger breast cancer tumors necessitate a mastectomy in every case?
A mastectomy is not necessary for all large tumors. The size of the tumor in relation to the size of the breast influences whether a lumpectomy or mastectomy should be performed during breast cancer surgery. If the patient had very large breasts, a 2-centimeter tumor would likely be manageable with a lumpectomy; nevertheless, if the patient had small breasts, a mastectomy would likely be advised.
Do older adults need to get a mastectomy if they have invasive breast cancer?
Mastectomy is one form of treatment for invasive breast cancer, but it isn’t always necessary, especially with all of the treatment options available today. The treatments your doctor prescribes, as well as their administration in what order, rely on a number of variables.
The patient and doctor together could decide the best course of action is to undergo chemotherapy first and then have a lumpectomy rather than a full mastectomy following chemotherapy if the tumor is small enough to do so.
New developments in breast-conserving surgery (lumpectomy) and mastectomy with reconstruction, such as oncoplastic breast reduction, nipple-sparing mastectomy, aesthetic flap closure, and other methods, can provide alternatives that preserve your appearance and self-image if surgery is the best option for you. Dr. Gorman always strives for breast-conserving surgery whenever possible.
Do older adults that have breast cancer need chemotherapy?
Although a chemotherapy regimen can be difficult, chemotherapy can be an effective strategy to shrink a tumor. However, chemotherapy may not always be required, depending on the patient’s particular circumstances.
The information obtained from the Oncotype genetic profile of cancer can help determine whether chemotherapy will be helpful in postmenopausal patients with invasive cancer whose tumor is larger than 1 centimeter and hormone receptor positive. Adjuvant chemotherapy may be associated with improved survival outcomes in elderly patients with breast cancer.
Even if elderly breast cancer patients have cancer in their lymph nodes, depending on the results of the tests, they may be able to forego chemotherapy in favor of hormone-blocking medication, which is easier to take and has fewer adverse effects. Hormone therapy can be given orally and spread out over five years.
Do all lymph nodes have to be removed if breast cancer has spread to them?
Not all the time. Fewer surgeries to remove axillary lymph nodes are currently being performed by surgeons. The risk of lymphedema was higher a few years ago when the recommendations were different, and breast cancer that had spread to the lymph nodes required the removal of every one of them.
Adjuvant radiation therapy to the residual lymph nodes has been shown in recent studies to be as effective as axillary lymph node removal at controlling local cancer in some patients with cancer in the lymph nodes.
Another method of avoiding axillary lymph node dissection is first to use chemotherapy to reduce the cancer’s size. Fewer lymph nodes may need to be removed if there is a positive response.
How common is triple negative breast cancer in older patients?
Triple negative breast cancer affects about 10% of older women with breast cancer. It is more common for elderly women to be diagnosed with a hormone receptor positive breast tumor.
What is the prognosis for invasive breast cancer in women aged 70 and up?
Although receiving a cancer diagnosis is frightening at any age, older people may feel more vulnerable. But there are reasons not to worry because, thanks to breast cancer research, treatment options have advanced greatly, especially with an early breast cancer diagnosis.
Most frequently, in individuals aged 70 or older, the invasive cancer is hormone receptor positive, indicating a slower-growing cancer and is diagnosed while it is still an early stage breast cancer.
The data shows that the majority of people who are treated for invasive breast cancer survive. Even if you are diagnosed later in life, you can still successfully complete your treatment, carry on with your life, and eventually pass away from causes unrelated to breast cancer. This is especially true for those who are capable of taking care of themselves and are in good overall health without another comorbidity at the time of their diagnosis.
Dr. Gorman is dedicated to offering patients of any age an advanced, personalized, and targeted approach to breast surgery and the treatment of breast cancer. Early detection is crucial when it comes to treatment options for breast cancer. Consult your doctor to discuss your symptoms and determine whether you require additional evaluation if you are concerned about any new changes in your breasts or possible breast cancer symptoms. To schedule a consultation with Dr. Gorman or to learn more information about breast cancer treatment, visit the Texas Breast Center website or call the office today.
Following a breast cancer diagnosis, medical professionals will look to see whether and how far the disease has spread. Staging is the term for this process. The cancer’s stage indicates how much cancer is present in the body. Determining the stage helps doctors evaluate the cancer’s severity and the most effective course of treatment. When discussing survival statistics, breast cancer doctors also refer to the stage of the malignancy. At Texas Breast Center, Dr. Gorman is dedicated to offering her patients the most advanced, personalized, and targeted approach to treating breast cancer with breast surgery. Her compassionate care, expertise, and dedication to continuing medical education make her patients feel at ease knowing she is on their team. To schedule an appointment with Dr. Gorman, call Texas Breast Center today.
What are the different stages of breast cancer?
Most patients want to know what their breast cancer stage is as soon as they receive the initial medical diagnosis of breast cancer. Breast cancer is understood to have five stages. The American Joint Committee on Cancer TNM staging system (AJCC cancer staging manual) is the staging method most frequently utilized for breast cancer. The most recent TNM system, effective January 2018, has both pathology and clinical staging systems for breast cancer.
Dr. Gorman will provide you with further information about the stage of your breast cancer when you speak with her at your appointment. She will take the time to thoroughly explain what your particular stage means, as well as listen to and answer any of your questions.
Stage 0
The earliest stage of breast cancer, also known as ductal carcinoma in situ, occurs when abnormal but non-invasive cells are found in the lining of the breast milk duct. There is no proof that the cancer has spread (metastasis), and it is still quite treatable at this point. This stage is also known as pre-cancer or early-stage breast cancer. Dr. Gorman will assist you in developing a treatment strategy.
Stage 1
In the next stage, there is undeniable proof of the presence of breast cancer cells rather than abnormal cells. The good news is that stage I breast cancer has a high chance of being successfully treated when diagnosed early and therapy is initiated.
Typically, Stage I is separated into stage Ia and stage Ib. Ia refers to a tumor size that is less than 2 cm in size and does not show signs of spreading to the axillary lymph nodes. When there is only a small amount of evidence of cancer in the breast and lymph nodes, but either no tumor is present in the breast tissue or the tumor is smaller than 2 centimeters, the diagnosis is Ib.
Stage 2
When cancer is identified as being stage II breast cancer, the tumor is larger and is still growing, but at this point, it is only inside the breast tissue or lymph nodes. Again, there are subsections for stage II that deal with the size of any tumor and whether or not there is spread to nearby lymph nodes. By its very nature, stage II cancer is considered invasive breast cancer and will require a more aggressive course of treatment than stage I cancer. However, the prognosis is still favorable, with excellent breast cancer survival rates, providing treatment is initiated early.
Stage 3
A stage III cancer diagnostic indicates that the tumor has spread to other areas of the body. At this point, it will not have started to affect other distant organs. Many oncologists classify this cancer as being “advanced.” The majority of recent treatment option developments have, however, made substantial strides at this stage. Chemotherapy and/or radiation therapy are potential treatment options at this stage.
Stage III cancer treatment is divided into two categories based on the severity of the disease and how many lymph nodes are involved. Some stage III breast cancer is also called inflammatory breast cancer. The tumor may just need to be shrunk with chemotherapy first, and if the patient responds well to the medication, breast cancer surgery may then be explored in the future. It’s crucial to keep an optimistic attitude and observe how your cancer responds to treatment.
Stage 4
Breast cancer that has reached stage IV has spread to other parts of the body and is also known as metastatic breast cancer. The brain, bones, thoracic wall (chest wall), sternum, skin, clavicle, liver, or lungs may be areas it has spread to at this stage. Stage IV breast cancer is often managed as a chronic condition because it is not thought to be curable. The outlook for many women is significantly better thanks to modern medical advancements, combined with a positive mental attitude and view on life. There is always hope at every stage because breast cancer research, clinical trials, and improvements in breast cancer treatment are continuous.
See the related article on Does Every Breast Cancer Patient Need Surgery?
More FAQ’s about Breast Cancer Staging
What procedures are used to determine the stages of breast cancer?
The following diagnostic tests can be used to determine the stage of breast cancer:
Mammogram
Breast MRI
Blood tests
Bone scan
PET scan
CT scan
Breast biopsy
Ultrasound
How fast does breast cancer spread?
All types of cancers are capable of spreading, but whether they do and how quickly they spread depends on a few different factors. The type of breast cancer you actually have is the main factor your doctor uses to assess whether or not your disease will spread quickly. Different breast cancers develop at varying rates. Given that every cancer diagnosis is unique, it is challenging to provide a general prediction of how quickly breast cancer may spread.
Finding the typical growth rate of breast cancer is as challenging as figuring out how long breast cancer takes to develop. The amount of time it takes for a tumor to double in size has been studied in many ways, but the results are highly variable depending on the type of breast cancer and the patient.
It’s difficult to pinpoint the exact rate at which breast cancer can grow and spread because different forms of the disease frequently exhibit varied characteristics. However, doctors are aware that some forms of breast cancer tend to be more aggressive and spread quickly, whereas other forms usually advance more slowly.
Generally speaking, the likelihood that your tumor will spread to neighboring tissue and other parts of your body increases as it grows. Several variables, including breast cancer grades, can affect how quickly your breast cancer grows. Special proteins called receptors have a role in the growth and survival of cancer cells. Breast tumors with hormone receptors, which depend on the growth hormone estrogen, progress more slowly than other types.
Other types, however, may be more aggressive and rapidly growing. These include triple-negative breast cancer, which lacks hormone receptors and HER2, and HER2-positive tumors (also sometimes referred to as HER2/neu proteins), which depend on a different type of protein for growth.
It is more likely that cancer that has spread to other places in your body will do so again. Your chance of the cancer spreading increases with the stage of breast cancer you have.
Can you do anything to prevent or slow the spread of breast cancer?
There is no guaranteed method for preventing breast cancer. However, there are certain things you can do to reduce your breast cancer risk. While breast cancer cannot always be prevented, it can occasionally be slowed down, prevented from spreading, or even have its size reduced. You can accomplish this by following all prescription instructions, completing all prescribed treatments, attending all scheduled visits with your oncologist or breast cancer surgeon, and actively participating in your breast cancer treatment.
Correct drug administration, a nutritious diet, regular exercise, and stress management are all things you can control. All of these things can help you become more physically fit and which leads to a more positive outlook on life, which can have a positive impact on your breast cancer diagnosis.
What are the survival rates at each of the breast cancer stages?
In the United States, non-metastatic invasive breast cancer patients have a 90% five-year survival rate. For women with non-metastatic invasive breast cancer, the ten-year survival rate is 84% on average.
Women with invasive breast cancer have a 99% five-year survival rate if the disease only affects the breast. Sixty-five percent (65%) of breast cancer diagnoses in women are at this stage. In the United States, women between the ages of 15 and 39 are less likely than women over the age of 65 to have their breast cancer detected at an early stage (68% of cases in this age range). This might be because, unless a person is at a greater risk, the majority of mammography and breast cancer screening doesn’t start until age 40.
The five-year survival rate is 86% if the malignancy has progressed to the lymphatic system. The five-year survival rate is 29% if the cancer has progressed to a distant area of the human body.
The likelihood of recovery for any given person is dependent on a variety of factors, including the size of the tumor, the number of lymph nodes that have cancer, and other characteristics of the tumor that affect how quickly a tumor will grow and how well the treatment works. It is important to remember that these statistics are averages. As a result, it can be challenging to calculate each person’s likelihood of surviving.
When it comes to breast cancer survival and the best treatment options, early diagnosis is crucial. If you have any concerns about recent changes in your breasts or possible breast cancer symptoms, speak with your doctor to discuss your symptoms and determine whether you require a physical examination, additional testing, or medical imaging.
Dedicated to giving her patients the finest care possible, breast surgeon Valerie Gorman, MD, FACS, puts all of her passion and determination into her work. She believes that treating every patient from the time of their initial diagnosis will provide her with a long-term perspective on their disease and how it is progressing. Dr. Gorman’s kindness and attentiveness are just two reasons that patients choose her for their breast cancer surgery. To request an appointment with Dr. Gorman, call Texas Breast Center or visit the website for more information.
National Breast Cancer Awareness Month is in October, and not only should you wear pink this month, but you should also learn what you can do to inform yourself, your friends, and your family about the risk factors and symptoms of breast cancer. It also involves offering assistance to those who have received a medical diagnosis of breast cancer, undergone breast cancer treatment, or lost a loved one to the disease.
Breast Cancer Awareness month aims to equip you with the tools you need to protect yourself, as well as with breast cancer information materials and support services. Breast cancer is the most common cancer in the United States, and early breast cancer detection is the key to saving lives. Texas Breast Center extends an open invitation to everyone to take part in Breast Cancer Awareness Month and urges women to self-examine their breasts and educate others in their communities about breast cancer prevention and risks.
The Benefits of Breast Cancer Awareness Month
Breast Cancer Awareness Month is more than just pink ribbons and is significant because it raises money for life saving research into the disease’s causes, treatments, and cure while also raising public awareness of the disease. It educates on the importance of routine breast screening and early detection.
Public education represents one facet of awareness. Campaigns for Breast Cancer Awareness Month assist in educating people about the warning signs and symptoms of the disease as well as preventative measures, such as how to do a self-exam, where to find the right breast cancer screening, and the value of routine mammograms. For those impacted by breast cancer, the month also spotlights cutting-edge, effective procedures and treatments, even those that may not be well-known to the general public.
Raising money for research is one of the other main objectives of Breast Cancer Awareness Month. Through various events organized throughout the month, including races, walks, social media campaigns, and others, participants are able to raise more money to fund life-saving research and continue creating innovative treatments that have improved outcomes, lowered the mortality rate over time, and given patients with the disease hope.
Most importantly, Breast Cancer Awareness Month is a time to honor the breast cancer survivors who battled the disease and to express support and solidarity for those who have been affected by breast cancer.
Early Detection
The growing participation in Breast Cancer Awareness month over the last thirty-plus years has helped increase awareness about the importance of early detection of breast cancer. Though it can affect women of any age, women over 50 are most frequently diagnosed with breast cancer. To find any early indicators and increase your chances of receiving successful treatment, it is crucial to regularly examine yourself and have your health assessed by a medical professional.
Every month, you should perform a breast self-exam. Lay down on your back and raise your right arm to conduct a self-exam. Check the entire right breast and armpit region with three fingers on your left hand for lumps, knots, or extra skin thickness. In the shower, you can also carry out this examination by elevating your arm above your head. It is also advised to check your breasts in the mirror to check for any visible symptoms like skin puckering or dimpling.
Self-examinations are helpful, but screening mammograms offered by healthcare providers are crucial for early diagnosis since they can identify breast abnormalities before a lump can be felt, which ultimately saves lives. Women 40 and older should get mammograms every year. Visit with your physician if you have a family history of breast cancer to evaluate the need for increased screening. An annual exam is also advised for women, especially if there is a family history of breast cancer. Routine mammography is one of the most crucial steps you can take to keep your health, prevent disease, and live a healthy life.
Lowering Your Risk
Even though there is no guaranteed way to avoid developing breast cancer, there are steps you can take to potentially lessen your risk. According to the breast cancer research of the American Cancer Society, there are several ways to lessen the risk you will develop breast cancer.
Maintain a Healthy Weight or Lose Weight if Needed: Breast cancer risk increases after menopause in adults who are overweight or obese. To reach or maintain a healthy weight, maintain a balance between your food intake and physical activity.
Keep Moving: Low risk of breast cancer risk is connected to moderate to vigorous exercise levels. Include 150 to 300 minutes a week of moderate-intensity exercise!
Limit Alcohol Consumption: Alcohol should be avoided or consumed in moderation as it raises the risk of breast cancer. Alcohol consumption, even at low levels, has been associated with an increase in risk. If you chose to drink alcohol, limit your consumption with this in mind.
Breastfeeding: The majority of research indicates that breastfeeding, particularly if it lasts for a year or more, may indeed reduce the risk of breast cancer.
In addition, taking hormone replacement therapy and some birth control medications (a combined oral contraceptive pill) have been linked to an increased risk of breast cancer.
Support for Breast Cancer Patients
While October is dedicated to raising awareness and preventing breast cancer, it is also a time for charities and organizations to promote the support services they offer to breast cancer patients and survivors. Pick your favorite non-profit organization or breast cancer foundation and make a financial donation to help further the work they are doing for Breast Cancer research and support. In addition to supporting a 501(c)(3) organization financially, you can also provide support to patients facing breast cancer.
There are numerous ways in which you can assist and support someone who has received a cancer diagnosis. Start by being there and providing a listening ear. Consider leaving a supportive note on someone’s CaringBridge page. Think about the assistance that a cancer patient’s family could find useful. You can either bring food or work with others to put together a group to provide food. You can send a note, leave your favorite book, or make a movie recommendation. Keeping in touch and showing support can mean the world to someone.
The success rates of breast cancer treatment continue to rise along with the amount of research being done. We recognize that a breast cancer diagnosis is personal and can still feel disorienting, despite advances in research. Texas Breast Center is dedicated to supporting you at every turn. Through a specialized, tailored treatment plan and ongoing support after your initial treatments, the team wants to establish a connection with you and give you hope.
Breast surgery expert Valerie J. Gorman, MD, FACS, focuses on surgical oncology and surgical diseases of the breast. You will have access to a wide range of treatment choices, including hormone therapy, while under her care, as well as a regimen of care tailored to your particular breast cancer.
Our goal is for each of our patients to go from being a breast cancer patient to a breast cancer survivor. Texas Breast Center is dedicated to promoting Breast Cancer Awareness in October and beyond by providing information, support, and more resources as we work together to save lives.
Many breast cancer patients wonder if surgery is always a required step in breast cancer treatment. In early-stage breast cancer, studies are finding that there are often breast cancer chemotherapy drugs and radiation treatments that are quite effective at eliminating cancer cells and reducing the amount of breast cancer surgery. At Texas Breast Center, our goal is to help patients find the most minimally invasive treatment with the best outcome for their particular type of breast cancer.
Dr. Gorman, as an experienced breast cancer surgeon, has a deep understanding of the benefits and downsides of surgery. Breast cancer surgery can significantly improve or greatly diminish a woman’s quality of life, sometimes without improving her long-term survival, depending on the particular circumstances surrounding the patient. The art of medicine and surgery for breast cancer is to match a patient’s goals and tumor features with the appropriate treatment strategy (such as chemotherapy, radiation therapy, hormonal therapy, surgery, or alternative medicine) in a way that maintains or improves cancer control while preserving or improving quality of life.
According to two new clinical trials, patients with early-stage breast cancer who respond well to neo-adjuvant chemotherapy or targeted therapy before surgery may be able to decrease the amount of surgery followed by radiation therapy, with a low risk of cancer returning. Dr. Gorman is dedicated to offering her patients an advanced, personalized, and targeted approach to breast surgery and the treatment of breast cancer. Call Texas Breast Center today to schedule a consultation and learn more about the types of breast cancer treatment we offer.
What is the de-escalation approach to cancer treatment?
In an effort to tailor the different types of treatments to a particular subtype of the disease, the de-escalation approach to cancer treatment focuses on using less treatment and fewer interventions to produce the same effects. If gene tests reveal that chemotherapy for breast cancer won’t be effective at reducing breast cancer cells and there are alternative cancer drugs available, some breast cancer patients may be able to skip chemotherapy, sparing them both short-term side effects and longterm effects.
De-escalation can also involve reducing surgery or performing a lumpectomy that preserves breast tissue rather than a mastectomy to treat breast cancer. The goal of de-escalating breast cancer treatment is to reduce morbidity and enhance the patient’s quality of life without jeopardizing the disease’s outcome.
Research on Chemotherapy as Breast Cancer Treatment without Surgery
Researchers at MD Anderson Cancer Center stated in a news release that “This research adds to growing evidence showing that newer drugs can completely eradicate cancer in some cases, and very early results show we can safely eliminate surgery in this select group of women with breast cancer,” said principal investigator Henry Kuerer, M.D., Ph.D. After receiving chemotherapy before surgery, patients who were thought to be in complete remission were examined by researchers to determine the likelihood of breast cancer reoccurring in these patients.
After a median follow-up of 26.4 months, the study found that 31 of the 50 patients who were tracked had a complete response to chemotherapy and none had a breast tumor recurrence. The study shows promise as a less invasive way to treat cancer, as these types of cancers usually recur within the first couple of years. According to Kuerer, “Patients often have surgery first, but these targeted therapies increase survival. So give it first — it shrinks tumors, allowing lumpectomy vs. mastectomy.”
50 women over age 40 with early-stage triple-negative breast cancer or HER2-positive breast cancer who had a breast lesion that measured less than 2 cm after receiving a conventional targeted chemotherapy regimen participated in the multi-center trial. Breast surgery was withheld, and patients continued with conventional radiation therapy if cancer was not found on biopsy.
The VACB classified 31 individuals among the participants as having a pathologic complete response, which means a pathologist could not find cancer in the tissue where the tumor was discovered. Even while the surgery-free plan seems to have been effective thus far, the trial only involved a limited number of well-screened women, who were observed for a median of 26 months. It’s a sizable amount of time, particularly for the particular breast cancer types analyzed, in which breast cancer recurrence frequently happens in the first several years. Experts agreed that a larger study with a comparison group would be necessary to determine whether changes in medical practice for the treatment of cancer are necessary, as the study was performed on a particularly small group. The study is a good start, but the results cannot be claimed as conclusive with such a small test group.
The chief executive officer of the American Cancer Society, Karen Knudsen, said, “What I really appreciate about the study is that it takes the next step and asks a bold question: How do we take all the advances that we’ve made in more tailored and specific cancer therapy, and convert that to reducing the number and types of interventions any one patient needs to incur?”
Utilizing every resource available in contemporary medicine is the traditional strategy for treating breast cancer. The removal of the tumor via surgery is seen as a crucially important step, along with radiation therapy for breast cancer, medication, hormone therapy, and, when indicated, immunotherapy to destroy cancer cells. It is especially important to utilize all of these interventions available when formulating a treatment plan to treat metastatic breast cancer as well as locally advanced breast cancer.
While the study results are quite promising and encouraging, it is important to note that more cancer research must be done before making this a part of routine breast cancer treatment protocols. Neoadjuvant chemotherapy treatments, or chemo drugs that are administered prior to surgery with the intention of having a less extensive surgical procedure, has become so advanced that oftentimes the cancer cells are gone before the time of surgery. With adjuvant therapy becoming more targeted and effective at treating breast cancer, there is great hope that in the future, surgery to remove breast cancer will be needed less often. The benefits of chemotherapy outweigh the risks, both physical and emotional, that are associated with surgery for many patients. Breast cancer patients should talk with their doctor to find out if neoadjuvant therapy would be beneficial for their particular type of breast cancer.
A breast cancer diagnosis can be alarming, which Doctor Gorman and her staff at Texas Breast Center are mindful of when providing compassionate care for patients. She is committed to providing her patients with a sophisticated, individualized, targeted approach to breast surgery and breast cancer treatment, along with top-tier treatment regimens. She never advocates for additional treatment that would be unnecessary for a patient but works to find the best possible treatment for the best quality of life and results. For in-depth information about breast cancer, risk factors, therapies for breast cancer, and preventive measures that can be taken, as well as to schedule a consultation with Dr. Gorman, visit the Texas Breast Center website.
The BioZorb® is a 3D implanted tumor bed marker created for patients with breast cancer to mark the breast cancer surgical excision site accurately. It consists of a spiral three-dimensional bioabsorbable framework embedded with six permanent titanium surgical clips. The BioZorb® offers 3-dimensional breast radiation treatment targeting and is available in various sizes from 2-5cm, including Lower Profile, and is intended to enhance results in breast-conserving surgery (BCS) when used in early breast cancer stages. Low Profile (LP) is an ideal option for smaller, flatter surgical cavities.
Dr. Gorman is one of the leading breast surgeons that has successfully used the BioZorb® implant in hundreds of Stereotactic Body Radiation Therapy (SBRT) breast cancer surgeries. She has seen firsthand how they improve outcomes with breast-conserving therapy post-surgically.
The BioZorb® implant has many benefits for patients, including excellent cosmetic outcomes, improved accuracy in radiation therapy, and minimal scarring after breast conservation therapy. Many breast cancer patients who have received breast-conserving surgery have experienced the benefits of the BioZorb® implant, though there have been a few reported side effects. This article will discuss some of the side effects reported by patients who have had the BioZorb marker implanted and how the benefits still outweigh any potential risks.
BioZorb® Reported Side Effects
Some patients with BioZorb® implants have reported hard, uncomfortable lumps in the area of their implants.
Patients have reported skin deformation and scarring of the skin around the devices.
Patients have reported skin reddening, irritation, and itching in the vicinity of their BioZorb® implants.
Patients have reported that the devices have not been absorbed in the expected time frame but instead have stayed intact for over 2.5 years.
Some individuals also claim that the implant is so unpleasant that they want it removed or decide to undergo partial breast reconstruction or a mastectomy to remove the entire breast.
Some patients report that the BioZorb® implant causes the affected breast to become noticeably bigger than the unaffected breast.
Do the benefits of the BioZorb® implant outweigh the side effects?
About 60% of the more than 200,000 American women with early-stage breast cancer had a lumpectomy with whole breast irradiation. Since it can be challenging to identify the specific region of the breast where the tumor came from, radiation is often applied to the entire breast. BioZorb® was developed to improve the accuracy of such radiation therapies, and it has done just that.
Six titanium clips on the device show radiation oncologists precisely where to point the radiation beam. Radiation is thus applied to the tissue that needs it the most. The “lumpectomy bed” will then benefit from the boost of radiation. And even though sometimes the whole breast must still undergo radiation treatment, BioZorb® guarantees that the correct location gets the optimal boost dosage. With BioZorb®, Dr. Gorman also has been able to use partial breast radiation with SBRT (BioZorb® as the target). This shortens the course of radiation to five days and has improved cosmetic outcomes.
According to a study in the World Journal of Surgery, of 110 patients using the BioZorb® implant, the marker enabled more precise targeting for radiation planning and treatments in 95.7% of the cases.
Over the course of around two years, BioZorb® is naturally absorbed by the body, but the titanium clips are left in place. As a result, during routine mammography, it is easier for your doctor to precisely analyze the former tumor spot.
Breast surgeons are utilizing an extra advantage of BioZorb® implantation. After surgery, the BioZorb® prosthetic implant aids in preserving the breast’s natural form by supporting the breast tissue. As part of your lumpectomy, the 3-D spiral design of the marker is proving to help reshape the breast, which enhances the breast’s contour and, ultimately, its aesthetic appeal.
Dr. Gorman and BioZorb®
BioZorb® provides breast cancer surgeons with another cutting-edge method to enhance therapeutic and cosmetic results and improve overall patient outcomes. Dr. Gorman believes that for many patients, the benefits of the BioZorb® device outweigh any potential side effects. She continues to perform surgeries with the BioZorb® implant to help more women heal and recover.
If you have questions about the BioZorb® device or breast cancer treatment, please call our office to schedule an appointment. At your consultation, Dr. Gorman will be happy to personally answer all of your questions. Texas Breast Center is committed to providing its patients with a personal, individualized, and targeted approach to breast surgery and breast cancer treatment.
Around the globe, breast cancer affects millions of women. One in eight women is predicted to have breast cancer during their lifetime in the United States alone. While there are several risk factors that you can’t control, such as a family history of breast cancer or dense breast tissue, there are certain behaviors and lifestyle choices that may have a significant impact on lessening your risk. Eliminating the habits that you can control can help decrease your risk of developing breast cancer.
Poor Diet
About 30 to 40 percent of all malignancies are considered to have some connection to diet. You cannot avoid developing breast cancer with diet or food alone. However, certain meals may improve your body’s health, strengthen your immune system, and lower your chance of breast cancer. According to research, eating a range of foods that are high in nutrients, including fruits, vegetables, legumes, and whole grains, may help you feel your best and provide your body with the energy it needs. Animal studies suggest eating food cultivated without pesticides may help prevent the unfavorable cell alterations linked to pesticide usage.
In nations where the traditional diet is plant-based and low in total fat, breast cancer is less prevalent. However, studies on American adult women haven’t shown a link between dietary fat consumption and a woman developing breast cancer. A high-fat diet throughout adolescence, however, may increase a girl’s risk of developing breast cancer later in life, even if she doesn’t go on to gain weight or become obese.
Further study is required to fully comprehend how nutrition affects the risk of breast cancer. However, it is undeniable that calories do matter, and fat is a significant source of calories. Being overweight or obese, which are breast cancer risk factors, may be brought on by high-fat diets. Because excess fat cells produce estrogen, which may promote the development of extra breast cells, overweight women are considered to have a greater chance of developing breast cancer. Breast cancer risk is increased by this additional growth.
Lack of Exercise
Regular exercise benefits your health in a variety of ways, one of which is a decreased risk of breast cancer. Over the last 20 years, several studies have consistently shown a relationship between increased physical activity and a decreased risk of breast cancer.
It is unclear exactly how exercise reduces the chance of developing breast cancer. It is believed that exercise controls estrogen and insulin, two substances that may promote the development of breast cancer. Regular exercise also aids women in maintaining a healthy weight, which supports hormone regulation and immune system health.
Unfortunately, there is no magic number of hours a woman should exercise each week to prevent breast cancer. We do know that more is preferable to less, and that some is better than none. Additionally, more intense exercise is more productive than less intense exercise. All people should exercise for at least 150 minutes per week of moderate effort or 75 minutes per week of vigorous intensity, ideally spaced out over the course of the week, according to the American Cancer Society.
Brisk strolling, dancing, leisurely biking, yoga, golfing, softball, doubles tennis, and routine yard and garden upkeep are some examples of moderate-intensity exercises. Jogging, running, rapid cycling, swimming, aerobic dancing, soccer, singles tennis, and basketball are some examples of high-intensity exercises. Along with your regular daily activities at home and at work, all of these extracurricular activities include stair climbing and walking from your vehicle to the garage.
Exercise has the additional benefit that it keeps you from merely sitting around. The probability of acquiring breast cancer and several other forms of cancer, as well as obesity, type 2 diabetes, and heart disease rises with sitting time, regardless of how much exercise you receive when you’re not sitting, according to an increasing body of research. Many of us spend most of our workdays seated at a desk. Because of this, it’s even more crucial to include activity throughout your day.
Certain Types of Birth Control
There is a small increase in the risk of breast cancer associated with the current or recent usage of oral contraceptives. According to studies, women’s breast cancer risk is 20–30% greater while using birth control pills (and immediately after) than the risk for women who have never used the pill. However, since the absolute risk of breast cancer for the majority of young women is low, this additional risk has only a little effect.
Women’s chances of developing breast cancer start to decrease after they quit using oral contraceptives. The risk eventually drops to the same amount as women who have never used the pill. Despite the increased risk of breast cancer , birth control pills also lower the risk of uterine and ovarian cancer in addition to preventing pregnancy. Just like with previous, higher-dose versions of the drug, modern, lower-dose tablets have been associated with an increased risk of breast cancer.
Some alternative contraceptives contain (or release) hormones, just like birth control pills do. Depo Provera users who have been using it for extended periods of time may be at a higher risk for breast cancer than women who have never used it.
Research on IUDs that release hormones and breast cancer research have conflicting results. IUDs don’t increase the risk of breast cancer, according to some research. According to other studies, women who use hormone-releasing IUDs may have a 20% greater chance of developing breast cancer (similar to birth control pills). According to other research, women who previously used hormone-releasing IUDs may be more likely to develop breast cancer after menopause.
Discuss the advantages and disadvantages of any contraceptive pill with your doctor before using it (or if you already are and haven’t done so).
Not Getting Routine Mammograms
Low-dose x-rays of the breast are called mammograms and can help doctors identify a breast cancer diagnosis. Regular mammograms are one of the best breast cancer screenings that may assist in detecting early stage breast cancer, when treatment has the best chance of being effective. Years before physical breast cancer symptoms appear, a mammogram may often detect breast abnormalities that might be cancer. Results from decades of research definitively demonstrate that women who receive routine mammograms are more likely to have breast cancer discovered earlier, are less likely to require an invasive breast cancer treatment like chemotherapy and surgery to remove the entire breast (mastectomy), and are more likely to recover from the disease.
Mammography is not flawless at detecting breast cancer cells. Dense breast tissue can make it harder for radiologists to see breast cancer on mammograms. Although most breast cancers will be detected, some will be missed. A woman will probably need more testing (such as additional mammograms or a breast ultrasound) in order to determine if anything seen on a screening mammogram is cancer. Additionally, there is a slight possibility of receiving a cancer diagnosis that, if not discovered during screening, would never have given rise to any issues. It’s crucial that women undergoing mammograms be aware of what to anticipate and the advantages and limitations of screening. As you age, your risk of developing breast cancer increases. Breast cancer screening through mammography is vital for women over age 40.
Use of Tobacco Products
According to research, smoking may significantly increase the chance of developing breast cancer, particularly in women who began smoking as adolescents or who had a family history of breast cancer. Smoking might increase one’s chance of developing breast cancer because specific chemicals in tobacco products may cause out-of-control cell proliferation in the body. Smoking is associated with an increased risk of breast cancer in certain women, despite the fact that it is not thought to be a direct cause. In addition, smoking may make treating breast cancer more difficult and lead to complications from breast cancer surgery. Avoiding tobacco products is an important factor in breast cancer prevention.
Excessive Use of Alcohol
Many studies reveal women who consume alcohol have an increased risk of breast cancer. According to research, the relative risk of breast cancer rose by roughly 7% for every alcoholic beverage taken daily. Compared to women who didn’t consume alcohol, women who had 2-3 alcoholic drinks per day had a 20% increased chance of developing breast cancer.
Alcohol may alter how a woman’s body processes estrogen. Blood estrogen levels may increase as a result of this. Women who drink alcohol have greater amounts of estrogen than non-drinkers do. As a consequence, higher estrogen levels are related to a higher risk of breast cancer. Alcohol and cancer risk can be controlled by limiting the amount you consume.
Hormone Replacement Therapy
Breast cancer risk is elevated by the majority of hormone replacement therapy (HRT) types. However, individuals who take combination hormone replacement therapy (HRT), which combines both estrogen and progesterone, are at a greater risk.
Breast cancer risk is only modestly elevated when HRT is used for less than a year. However, the hazards become more severe and continue longer the longer you use HRT.
HRT-related breast cancer risk varies from individual to individual. The risk may vary depending on your age when you start HRT, any medications you may be on, and overall health.
Breast cancer risk factors are greater for people who take HRT before or shortly after menopause as compared to those who start it later.
Even though there are several potential causes of breast cancer, some behaviors and lifestyle choices may have a big impact. These lifestyle choices, including smoking, drinking alcohol, and eating poorly may all raise your risk. Regular physical activity and maintaining a healthy weight are effective methods to lower your risk. This disease may also arise as a result of certain birth control methods and hormone replacement therapy. If you have any of these risk factors, it’s important to speak to your doctor about them.
Dr. Valerie Gorman, MD, FACS, a Waxahachie-based breast surgeon specializing in surgical oncology and surgical diseases of the breast, was selected for faculty at the prestigious Women in Breast Surgery conference. The Tampa, Florida-based conference was sponsored by Hologic, a groundbreaking enterprise designed to support women’s health by providing effective, state-of-the-art technology to healthcare professionals. Hologic constructed this two-day conference around the personal and professional development of women breast cancer surgeons.
Four renowned female surgeons, including Dr. Gorman, led the courses, merging the medical field and the business world through incorporating topics such as improving workflow efficiency, leadership and a seat at the table, getting the word out to build your brand, and offering a negotiation workshop. Dr. Gorman and her peers, who came from all over the United States, provided new breast surgeons and breast fellows (the medical community’s term for surgery residents and breast fellowships) with leadership and marketing tactics. “It was an honor to be a part of this,” said Dr. Gorman, “and to provide the tips and tricks I wish I had known when I was starting in the field rather than learning these strategies the hard way. This is really exciting work for the breast surgeon community.”
Educating the medical community on breast cancer surgery practices
Breast cancer technology
Gorman’s practice, Texas Breast Center, is considered a center of excellence for training among medical personnel. The conference’s sponsor, Hologic, sends its representatives and other physicians to be trained by Dr. Gorman and her team on the technology of the BioZorb, a marker device used for stereotactic body radiation targeted therapy, and the wireless technology she employs. Dr. Gorman is grateful for the opportunity to train other physicians and industry persons on breast cancer treatment and care advancements. “Bringing them into the process of these surgical techniques and utilization of the BioZorb to gain a first-person understanding of the tools they are selling or using is essential to promoting healing and recovery for patients; education is key,” emphasizes Dr. Gorman. Her desire to raise awareness and educate others in the field led her to present at the Women in Surgery conference.
Strategies for breast surgeons
Dr. Gorman emphasizes the importance of empowering women, physicians and patients alike, through education. Her presentations at this conference aimed to help women claim their spot at the table among the leading breast cancer surgeons by providing insight into the business side of surgery, an aspect that is often neglected within the medical field. Additionally, effective business tactics would lead to larger public exposure of surgeons and, thus, more conversations surrounding breast cancer and breast care in general. Through a nationwide increase of young women entering the field with successful business strategies and tailored care for patients enduring breast cancer surgery, Dr. Gorman hopes this will lead to greater self-awareness and detection of early-stage breast cancer among the public.
Why is breast cancer awareness critical?
Breast cancer is one of the most common cancers detected in females, ranking second only under skin cancer. This means that, statistically, most women will either be diagnosed or know someone who has been diagnosed with breast cancer. Awareness helps us begin to topple this statistic. It leads to more women participating in self-checks, earlier detection, and an understanding of the risk factors that may indicate breast cancer. Opening the door for these actions to become regular practices starts with preparing and enabling newer breast cancer surgeons with the information surrounding strong business tactics and state-of-the-art care for patients and their communities. The Hologic Conference on Women in Breast Surgery sought to jumpstart these efforts, aligning with Dr. Gorman’s mission.
March is officially known as Women’s History Month! To celebrate women, the incredible things they have endured throughout history, and to highlight the value of their wellbeing, let’s examine breast cancer awareness throughout history. You are likely to see an influx of this information during October, but Dr. Valerie Gorman of Texas Breast Center emphasizes the importance of breast cancer awareness year-round. Doctors and breast care specialists universally agree that awareness of the realities and risk factors is critical in conquering breast cancer’s devastation.
While the history of breast cancers presumably goes back to the early days of humanity, widespread advocacy for the cancer community and dispelling the shame around breast cancer has had a much shorter timeline. Not only that, but common awareness of this cancer and its symptoms has just become prevalent within the last 50-75 years. Texas Breast Center wants to highlight the journey of awareness for breast cancer and, through doing so, encourage people to check their own breasts and to spread knowledge of both prevention and risks of breast cancer in their communities.
The Origins of Breast Cancer Awareness
When did breast cancer awareness begin?
Women have been at the forefront from the beginning of cancer research initiatives. Early forms of the American Cancer Society founded the Women’s Field Army, giving thousands of women the chance to instigate fundraising and promote research during a time when society handed them few other privileges.1 Despite the advancement of fundraising efforts beginning in 1913, discussing cancer was taboo and deemed unfit for conversations far into the 1900s. Particularly regarding breast cancer, public discourse would identify it solely as a “prolonged women’s disease.”2
Only in the 20th century did breast cancer finally reach public notice. This shift can largely be attributed to former First Lady Betty Ford. She opted for total transparency in her battle against breast cancer during the 1970s, a time when stigmas surrounding breast cancer were a crippling concern for many women. Using her platform, Betty Ford shared the importance of screenings, breast cancer treatment, and solidarity for other American women affected by cancer. This instigated a dramatic reformation in culture surrounding breast cancer, both in the societal support of breast cancer patients and in prioritizing regular doctor exams.
When did widespread breast cancer initiatives arise?
Recognition of the disease began at an individual level first, with women such as Betty Ford speaking candidly about their experiences. From this stemmed the opportunity for structural and organizational levels of awareness to be formed. The best-known cancer charity initiative is the internationally recognized Breast Cancer Awareness Month, taking place annually in October. In 1985, Imperial Chemical Industries and the American Society for the Control of Cancer partnered to create the first national week-long breast cancer awareness event. The initial intent of this was to encourage women to get regular mammograms, a form of breast imaging used to screen for breast cancer. This week later transitioned into a month-long observance of breast cancer survivors and patients.
Nowadays, it is incredibly common for a non-profit organization or a corporation to take part in the annual commemoration. From the NFL to cosmetic companies like Estee Lauder to The White House, public awareness campaigns, donation drives, and stories are spread to raise money and support systems for women who have been diagnosed with this disease. Estee Lauder created one avenue of this in 1992, seven years after the first awareness event, with the pink ribbon, and gave out over a million to initiate a tangible representation of the month’s efforts.3 This image is still easily identified today, commonly known as a symbol of support for patients.
The Importance of Breast Cancer Awareness
Why is breast cancer awareness so important?
Breast cancer awareness is crucial because of the approximate 13% chance of women receiving this diagnosis. (1 out of 8 women in America develop breast cancer at some point in life, with the likeliness increasing with age.) Knowing the statistics surrounding developing breast cancer, keeping watch over the risk factors, and seeking transparent, expert education on the latest prevention methods can help one improve their chances of keeping a late diagnosis at bay.
What are the achievements of the breast cancer movement?
Breast cancer research
An increase in awareness has led to a greater emphasis on research to cure breast cancer throughout recent history. Following individual concerns, support groups were created, leading to lobbyists and activists pushing for greater research and education on the disease. The Journal of Women’s Health provides one example of this through the seven-year project on environmental toxins and impact conducted by the Breast Cancer and Environment Research Centers (BCERC).4 This program was an influential precedent, as it was the first National Cancer Institute funded initiative to incorporate activists into the scientific research council. In this, those involved in pushing to raise awareness had a direct impact on the focus of the studies. This 2003-2010 project is simply one of many historical examples where voices in the community resulted in an incredible impact on cancer research. What proof that individuals’ involvement matters!
What is the aim of breast cancer awareness?
You Can Help Save Lives
Breast cancer is the second most common cancer in women. This means the odds of you or a loved one needing to be treated are high. Awareness aims to help eradicate this statistic, and you can play a tremendous role in this by educating yourself and your community on the risks. Being informed is crucial for many reasons, mainly because it teaches people about the necessary aspects of breast care. These are measures such as routinely scheduled mammograms, conducting self-examinations, maintaining a healthy weight, limiting alcohol consumption, pumping your own breast milk, extensively researching birth control pills and medicine, and staying active to the best of one’s abilities. Each of these factors can lead to a lower risk for women of developing breast cancer, or, if one is to get cancer despite a lowered risk, to an early diagnosis, which has proven to yield better outcomes.
Additionally, in creating ordinary spaces for conversations about the realities of breast cancer to occur, the perception of those whose lives have been affected by this disease will change for the better. Increasing knowledge in your community can breed hope and support for women with breast cancer. This acceptance can also lead to a society that encourages scheduling screening mammograms regularly, producing more cases of early detection, which can save lives.
Support for You
As research increases, so do the success rates of treatment. Even with improving science, we understand that a breast cancer diagnosis can still feel overwhelming. Texas Breast Center is committed to being with you every step of the way. The team aims to connect with you to provide hope through a personalized, targeted treatment plan and support that goes beyond your initial treatments. Valerie J. Gorman, MD, FACS, is a breast surgeon specializing in surgical oncology and surgical diseases of the breast. Under her care, you will find a broad spectrum of treatment options, such as hormone therapy, and a treatment program designed to benefit your exact case of breast cancer.
Lerner B. Inventing a curable disease: breast cancer control after World War II. In: Lerner B, editor. The Breast Cancer Wars: Fear, Hope, and the Pursuit of a Cure in Twentieth-Century America. Oxford: Oxford University Press, Inc.; 2001. pp. 41–68.
Ross W. Transformation. In: Ross W, editor. Crusade: The Official History of the American Cancer Society. New York: Arbor House; 1987. p. 33.
Officially recognized in 1976, February is dedicated as Black History Month in the United States of America. Commemorating the victories and legacies of African Americans and recognizing the hardships they have faced throughout our history, it is a pinnacle time of awareness and memorialization in the lives of American citizens. In honor of this past month’s observations, we wanted to provide information on women’s health surrounding the realities of breast cancer for black women.
Black Women and Breast Cancer
According to the American Cancer Society, breast cancer is the most commonly diagnosed cancer for black women. Falling second to lung cancer, breast cancer is also a top cause of cancer-related mortality. It is crucial for black women to understand the likelihood of a diagnosis, the risks surrounding breast cancer, and ways to routinely check for potential breast tumors. There are many questions surrounding the truth on breast cancer statistics, particularly pertaining to black women. Educating people on the realities of breast cancer plays a key role in women knowing what to watch for regarding their breasts and in changing some of the socially constructed elements surrounding medical and breast care for black women.
What is breast cancer?
Essentially, breast cancer is the uncontrolled development of breast cells. This is why it is recommended that women examine their breasts regularly for evidence of changes to the breast such as puckering or discoloration, as they are often the first symptoms to appear.
What would lead to a breast cancer diagnosis?
Although there are many different varieties of cancer, tumor biology at its base level remains consistent, and they all have similar characteristics. The genes in the human body regulate and control cell proliferation. The job of genes, which are found in the nucleus of cells, is to ensure that as old cells die, they are replaced by new cells. Mutations can develop, causing this process to be disrupted. This change can significantly affect the regeneration process, removing control from the genes and allowing the cells to continue making new cells without restriction. The production of additional cells can lead to the formation of a tumor. The emergence of a malignant tumor (which is an aggressive form of cells and can spread to other areas of the body via the blood and lymph systems) is what typically generates a breast cancer diagnosis.
Breast Cancer Risk for Black Women
Age, ancestry, family history, and type of diagnosis affect the severity and likeliness of breast cancer.
Who has the highest risk of breast cancer?
Despite a lower incidence of breast cancer development, black women’s lives are approximately 40% more likely result in breast cancer death. Women of a younger age, meaning below the age of 45, also tend to have the highest risk. There is no simple answer to this disproportion, as these starkly contrasting numbers seem to arise from a combination of factors, including both sociological conditions and genetic factors.
Disparities of Breast Cancer and Race
In recent years, there have been increasing conversations surrounding the tragic breast cancer disparities of medical care and attention for people of color. These risks and realities prove particularly tangled and problematic in the world of health care and surgical access. While this is true, Dr. Gorman of Texas Breast Center is eager to dismantle this problem through targeted, attentive care for each person who comes under her expert care.
The prevalence of breast cancer is still far greater than we like to see, which is why Dr. Gorman and her team at Texas Breast Center fight endlessly to see these numbers decrease. Particularly among black women, the statistics of more aggressive forms of breast cancer diagnoses, such as triple-negative breast cancer, are astronomically higher.
What is triple-negative breast cancer?
Triple-negative breast cancer is a form of breast cancer that tests negative for all three receptors: estrogen, progesterone, and HER-2. This kind of breast cancer is one of the more aggressive and invasive breast cancer types, with high spread and growth rates. Both age and race play into the likeliness of this diagnosis, as it is most common in women under forty and in black women.
Not all black women are at the same risk of developing triple-negative breast cancer. Research shows that particularly those born in Western Africa and the United States are at an increased risk for triple negative breast cancer in comparison to those born in East Africa. This difference is especially notable when compared to white women or women of other races. According to the American Cancer Society, black women in the United States are actually twice as likely as white women to receive this diagnosis. This may be a reason for the lower rate of survival among black breast cancer patients. Educating oneself on the risks of breast cancer can help black women act in anticipation and preparation and increase the chances of survival through early detection.
Dr. Gorman at Texas Breast Center
While statistics surrounding breast cancer can seem overwhelming and may evoke fear, Dr. Valerie Gorman combats this with the truth that “treatment for breast cancer has improved significantly over the last few years, and success rates continue to rise.” Breast cancer outcomes and treatments have never seemed more optimistic.
Dr. Gorman and her team at Texas Breast Center, located in Waxahachie, are devoted to caring for every patient in a manner tailored to their unique case, conducting each interaction with expert care, attention, and skill. Providing honest, advanced information on the risk factors of breast cancer and the leading treatment options is a top priority of this Texas-based breast surgeon. She dedicates herself to the wellbeing of every single patient and, in doing so, aims to topple the disparities that black women diagnosed with breast cancer face and help reduce the rates of breast cancer mortality, one case at a time.
Staying informed
As a leading surgeon, Dr. Gorman advocates for preventative measures and staying on top of breast health. Regular self-breast checks, mammography screening, a regular clinical breast exam, assessing controllable risk factors, and remaining informed on the latest news surrounding breast care are all steps that can increase the chances of detecting breast cancer while it is still in the early stages.
If you have any questions surrounding breast cancer or breast cancer risk factors, don’t hesitate to contact Dr. Gorman and her team at Texas Breast Cancer.
No one is excited to get a mammogram or go through other breast cancer screening tests. However, keeping on top of breast health and regular screening can be life-saving. The sooner breast cancer is diagnosed, the better the outcome is more likely to be.
First Steps
Keeping on top of regular breast self-checks, yearly mammograms, and annual physicals can help increase the chances of finding breast cancer in the early stages. That is to say, mammograms and self-checks will not increase the chances of a diagnosis but of early detection of the disease should it occur. These are three possible first steps in a potential breast cancer diagnosis.
Self Breast Check
A self breast-check, also known as breast self-exams, is a method used to keep yourself informed and aware of your own breasts and breast tissue. They should be done monthly, if possible, and especially if you meet a high number of risk factors, and they do not take long. But if performed regularly, they can keep you very familiar with the feel and appearance of the breasts, meaning any change is sure to stand out.
The process is relatively simple:
Start by looking at your breasts, both looking down and checking them in a mirror. Check for any changes in color, size, or shape. Signs of cancer or other infection are swelling, redness, dimpling, puckering, or discoloration. Especially check the nipple for inversion, pain, or unexpected or bloody discharge.
Raise your arms and reexamine. Having your arms up may shift the positions of the breasts to reveal something you may have missed otherwise.
Use the pads of a few fingers to carefully feel over the entire breast. Use consistent, small, circular motions to move across, up, and down the whole breast, covering the collarbone to the top of the rib cage and cleavage to the armpit
. Use enough pressure to feel deep tissue but not enough to hurt yourself.
Lay down and repeat the process.
Keeping up with regular breast self-exams will make it easier to notice any changes. If you find anything of concern, speak with your physician to discuss options and further screening.
Clinical Breast Exam
A clinical breast exam is part of the standard physical. It is a breast exam performed by your doctor, in which they will physically examine and feel each breast to feel for any changes or lumps in the tissue. The clinical breast exam becomes particularly relevant if you are at high risk of breast cancer or have noticed changes in your breasts during a breast self-examination. Raise any concerns with your physician so they can help you and discuss any necessary next steps.
It is not as simple as finding a lump and having doctors diagnose breast cancer. Should something be found during these exams, your doctor will likely send you to get a mammogram or ultrasound.
Schedule your appointment for a clinical exam today!
Another way to keep on top of your breast cancer risk and status is to receive regular mammograms. A screening mammogram, or mammography, is an X-ray of the breast using a low dose of radiation. Two plates will compress the breast at different angles to get multiple digital images, which a radiologist can examine for signs of breast disease or any other possible abnormality.
However, those who have particularly dense breast tissue or scar tissue in the breast are likely to have false positives in a mammogram. Breast cancer, dense tissue, and even cysts (fluid-filled sacs) appear white on x-rays, with limited ways to distinguish between them. For this reason, a potential positive from a diagnostic mammogram is not considered conclusively positive. Additional tests or a biopsy should be taken to confirm accuracy.
Ultrasound
A breast ultrasound uses sound waves to form a picture of the breast tissue. This is a good alternative to a mammogram if you’re pregnant and shouldn’t be exposed to x-rays. While ultrasounds are not generally used for cancer screening, they work well at differentiating a fluid-filled cyst from more solid masses. It can also give locations of tumors to help doctors, should they need to perform a biopsy or further investigation. Some surgical oncologists will use ultrasound during lumpectomies to establish the boundaries of the breast cancer before they begin removal.
MRI Scan
MRIs, or Magnetic Resonance Imaging tests, use magnetic fields to produce images of the breast’s interior. A contrast dye is injected before the screening, revealing where any blockages are. MRIs are not often used to diagnose breast cancer but instead used after an initial diagnosis to see how far cancer has spread. However, it can be used in combination with a mammogram to screen if:
there is a strong family history of breast cancer or ovarian cancer
the breasts are particularly dense (primarily ducts, fibrous tissue, and glands, with little fatty tissue), so any signs of breast cancer would be difficult to spot on a mammogram alone
the BRCA1 or BRCA2 gene mutation or other genetic mutations are present
radiation treatments have been applied to the chest before age 30
These traits can potentially lead to a high risk of breast cancer or, in the case of the dense tissue, an increased risk of missing early-stage breast cancer.
Metastatic Breast Cancer Detection
Specific imaging tests can detect metastasis once breast cancer has already been diagnosed. Biopsies can be performed by interventional radiologists, doctors whose primary focus is minimally invasive and targeted therapy.
Biopsy Sample
There are multiple kinds of biopsies, each serving their own purposes, though generally speaking, a biopsy is used to confirm or rule out a breast cancer diagnosis. Put simply, a biopsy takes a small amount of cells or tissue from an area of concern to examine under a microscope to establish whether these cells are cancerous or not. A pathologist–a doctor specialized in interpreting lab data and evaluating and diagnosing based on cells and tissues–will create a pathology report to explain what was found and discuss potential treatment options.
Fine Needle Aspiration Biopsy
The tissue or cell sample is removed using a thin needle.
Core Needle Biopsy
Like the fine needle aspiration method, the core needle biopsy uses a needle to remove the needed sample. However, the needle gets a core of tissue, so it collects a larger sample. This is generally the preferred technique for getting breast cancer diagnosed once an abnormality has been found in the breast, whether through physical examination or imaging tests. A pathologist will examine the sample to establish whether they are invasive cancer cells and identify any cancer biomarkers. Local anesthesia is commonly used to minimize discomfort during the procedure.
Image-Guided Biopsy
Image-guided biopsies are a form of core needle biopsy that map the area and guide the needle to the correct area of calcifications or mass through the use of imaging devices, such as ultrasound, mammography, or MRI. Usually, a marker is left behind–a small metal clip, usually titanium–to mark where the sample was taken.
Surgical Biopsy
Surgical biopsies are usually performed after a diagnosis has already been given, so they are rarely used as diagnostic tests. Most potential breast cancer patients will be given a form of needle biopsy to avoid unnecessary surgery. However, surgical biopsy does yield the largest amount of tissue.
Sentinel Lymph Node Biopsy
Breast cancer will sometimes spread into the local lymphatic system. The lymph nodes the breast cancer cells reach first are referred to as the sentinel lymph nodes and are usually the axillary lymph nodes (found under the arms). The sentinel lymph node biopsy removes 1-3 lymph nodes to avoid needing to remove more lymph nodes later.
Staging Breast Cancer
Once a breast cancer diagnosis has been established, your doctor will establish its severity in one of the breast cancer stages. The stage helps determine your prognosis and the best treatment options to take moving forward.
Some procedures that may be used to establish the breast cancer’s stage are:
Mammogram
Breast MRI
Blood tests
Bone scan
PET scan
CT scan
The stages ran from 0–meaning noninvasive and relatively contained–to IV–also called metastatic, meaning it has spread to other parts of the body.
Treatment Options
A patient’s treatment plan will be determined based on their breast cancer stage, health, and other factors. Dr. Gorman at the Texas Breast Center always ensures that each patient receives a personalized and targeted approach to breast cancer treatment to best meet their needs.
In layman’s terms, breast cancer recurrence happens when cancer has come back after treatment. When a number of breast cancer cells evade initial treatment and later aggregate, they cause the cancer to return despite months or even years of remission. It is important to note that a minimum of a year must pass between the execution of cancer therapy and the appearance of growing cancer cells for the growth to be deemed a recurrence, rather than treatment failure or progression of cancer.
Every survivor of breast cancer faces a chance of recurrence, so it is essential to understand what to look for and how to take proactive measures. We have written a previous article that details risk factors of breast cancer recurrence and many of the prevention and treatment methods used to fight the growth of cancer cells. However, new data has arisen, giving us an even greater insight into the ins and outs of breast cancer recurrence.
New Data
Initially, recurrence was thought to happen within the first five years after treatment. Risk is greatest during these beginning years, but up-to-date studies reveal that the risk of recurrence lasts more than thirty years. Cancer cells can lay dormant, causing them to be undetectable for long periods, leading to a recent notable concern of the risks of late recurrence. The growing concern is attributed to a high cumulative incidence increase (which is an estimate of the risk that one may experience an event within a specific period). This means that more patients are at risk for late recurrence due to an increased number of long-term breast cancer survivors.
While this information seems alarming, and certain factors make recurrence more likely, thankfully, those who have a recurrence are not in the majority, and research has allowed us to identify the most prominent contributors to recurrences. The study also notes that because of the allotted time between the research participants’ first diagnoses and present day, as well as the study’s focus on late recurrence (requiring an extended follow-up), there have been significant changes and improvements in treatment procedures and technology since the participants’ initial treatment. Therefore, the study results are uncertain in association with today’s regimens. Because of this, such studies are paramount and must be completed repetitively to find continual up-to-date results.
Recurrent Breast Cancer
While the chances of a recurrence are not common, it is still valuable to consider the risk factors and to understand the realities of the different types of recurrences.
Types of Recurrence
If a recurrence does occur, a breast surgeon will categorize it by its appearance in proximity to the initial breast cancer. The three forms are:
Local recurrence
This refers to when the breast cancer returns to the same chest area as the original tumor.
Changes in appearance or feel (such as thickening of the skin or new lumps) are typical indicators of a local recurrence.
Regional recurrence
It is deemed regional recurrence if cancer cells show growth in nearby lymph nodes (found in the armpit or collarbone) to the initial cancer area.
Regional recurrence is differentiated from local recurrence solely because of the involvement of lymph nodes.
Symptoms of regional recurrence may involve newfound pain or lumps in the arm attached to the side of the body with the original breast cancer.
Distant recurrence
When cancer has traveled to different parts of the body (such as bone or organs), it is considered a distant recurrence.
Another name for this is metastatic breast cancer.
Bone pain, weakness, and extreme fatigue may point to metastatic breast cancer.
It is considered stage IV cancer, as the cancer has extended to other parts of the body.
Which breast cancer is most likely to recur?
The initial diagnosis is a significant indicator of the chance of recurrence. Recurrent breast cancer is most likely to appear in patients who had an original tumor with more than three positive lymph nodes.
What are the chances of recurrence of breast cancer?
The cumulative incidence of recurrence is between 8.5-16.6% for fifteen to thirty-two years after a primary diagnosis. Chances of late recurrence are typically higher for those whose initial breast cancer was found in the lymph nodes and resulted in tumors over 2o millimeters. The chances are higher for women who were 35 or younger during their primary diagnosis. According to the recent data, 2,595 of the 20,315 women involved in the research study were diagnosed with a recurrence more than ten years following their initial bout with breast cancer.
Is recurrent breast cancer worse?
Recurrent breast cancer may prove more challenging to manage, and the therapy used in your initial treatment may no longer be effective in your specific case. Metastatic cancer may also require more aggressive treatment, as the cancer has spread to more than just one part of your body. Recurrent breast cancer should not automatically be considered worse than the primary diagnosis, but it will often require different methods of treatment or therapy.
Treatment
Even simple cells can become tumors if not adequately treated. It is impossible to guarantee a 100% chance of freedom from cancer recurrence. Still, treatment may be able to halt the growth of undetected cells for many years, and there are methods of prevention that the doctor-patient duo can take to reduce your risk of recurrence.
While a breast cancer diagnosis can seem bleak, both Dr. Gorman and the researchers of this recent study recognize the significant evolution of modern-day regimens and their success rate. If your breast cancer comes back, treatment is available. Depending on the type of breast cancer, treatment may entail surgical treatment and radiation therapy. More aggressive treatment regimens and therapy approaches may be merited for those at a higher risk of late recurrence. Survivors are also encouraged to stay under extended surveillance by making regular check-ins with their doctors and surgeons.
Risk Factors and Therapy
The chances of recurrence are significantly lowered by the proactive utilization of hormone, chemo, or radiation therapy following the initial removal of cancer cells. You can play a role in lowering the recurrence risk factors by opting for therapy options (such as radiation treatment or endocrine therapy) recommended by your oncologist. Such regimens may attempt to prevent breast cancer recurrence or aid in reducing the potential of recurrence. Exercise and a healthy diet are also easy, proactive measures to implement for holistic well-being and to reduce the risks of recurrence.
Dr. Gorman and Texas Breast Center
Remember that recurrent breast cancer is not your fault. Though a breast cancer diagnosis can be alarming or dismaying, Dr. Gorman holds fast to the fact that “treatment for breast cancer has improved significantly over the last few years, and success rates continue to rise.” There is great hope. Dr. Gorman understands the significant emotional and physical impact a breast cancer diagnosis can play in one’s life. Her team at Texas Breast Center is dedicated to offering patients personalized, advanced care in the treatment of breast cancer recurrence and the prevention of recurrence, as well as support that lasts long after your treatment regimen.
Breast cancer is represented by the pink ribbon. Research is fundraised through walks decked out in pink, and breast cancer awareness gear can be found covered in slogans like “big or small, save them all” or better yet, “fight like a girl.” And while the runs, marches, and merchandise can go a long way in raising money, they can also go a long way in implying some wrong information. If nearly all breast cancer awareness is geared towards women, does that mean men cannot–or do not–get breast cancer? No. Men may be less likely to get breast cancer than women, but there is still a risk.
How can you tell if a guy has breast cancer?
Breast cancer in men displays similarly to how it does in women. The symptoms are the same, and some are even more easily found due to the smaller amount of breast tissue in most men. With less breast tissue, lumps are more easily noticed and, therefore, diagnosed.
The most common symptoms of male breast cancer are:
Scaling, flaking, or redness of the skin of the nipple; can show as puckering or dimpling as well, or can happen to the skin over the whole breast, not just the nipple.
A painless thickening, swelling, or lump in the breast.
Nipple discharge, retraction, or ulceration.
Pain or pulling in the nipple area.
If the cancer cells spread further than the initial breast tumor, there can be additional symptoms and side effects, such as:
breast pain
bone pain
swelling in the underarm lymph glands
If anyone, no matter the person’s gender, experiences these symptoms, they should speak to their doctor. The sooner any breast cancer cells can be found, the more likely any treatment options are to work, and the less rigorous treatment needs to be.
How common is breast cancer in men?
While it is commonly known that breast cancer will develop in approximately one in eight women over the course of their lifetimes, the statistics on male breast cancer are less well known. When you search google for ‘how common is breast cancer,’ every answer on the first page is about women. Most sites collecting data on cancer categorize breast cancer as ‘female breast’ cancer to clarify that their data does not include men, despite many other cancer types (stomach, colorectum, leukemia, etc.) gathering data for both men and women. While this makes it easy to do cancer research for women, it makes it difficult to find information for male cancer patients.
One source, however, found that one out of every one hundred breast cancer diagnoses is given to a man. So, while men are at less of a risk than women, there is still a chance of breast cells becoming cancerous.
The American Cancer Society did offer that approximately 2,550 new male breast cancer cases are diagnosed each year. With breast cancer being 100 times more common in women than men, and with a man’s risk of diagnosis averaging around one in 1,000, it is easy to see why it’s not as prominently discussed. However, the risk is still there, and men should know what to look for to minimize risk.
However, just as with women, some men have more risk factors than others. These risk factors do not guarantee that this person will get breast cancer, nor does avoiding the risk factors guarantee that the person will avoid a breast cancer diagnosis. However, if you have these factors in your history, or are aware of them, be mindful of the signs, symptoms, and possible screening guidelines for breast cancer.
What are the risk factors for men?
Some of the risk factors for male breast cancer include:
Family history of breast cancer–you have a higher chance of developing breast cancer if you have a close family member who has, or has had, breast cancer.
Age–most male breast cancer diagnoses happen after 50 and are most commonly between age 60-70. It is usually rare for a man to get breast cancer under the age of 35.
Radiation therapy treatment–having a history of radiation therapy to the chest can increase the risk of breast cancer.
Liver disease–liver cirrhosis and other liver diseases can reduce androgen (commonly referred to as male hormones) levels and increase estrogen (commonly referred to as female hormones) levels in men, increasing risk.
Testicle surgery or disease–surgical removal of a testicle (orchiectomy), testicular injuries, or testicle diseases or conditions such as mumps orchitis or undescended testicles can increase breast cancer risk.
Estrogen exposure–those who take, or have taken in the past, estrogen or estrogen-related drugs (used for hormone therapy for prostate cancer) can have a higher risk of breast cancer.
Obesity–obesity can be associated with higher estrogen levels, leading to an increased risk factor.
Enlarged breasts–having enlarged breast tissue, known as gynecomastia, can come from infection, drug or hormone treatments, as well as other causes. Having additional tissue can make it difficult to notice early signs of breast cancer.
Breast cancer genes–mutations to the BRCA1 and BRCA2 genes dramatically increase the risk of breast, ovarian, and other cancers. People of all genders should be aware of the potential danger of the mutation of these genes.
Klinefelter’s syndrome–Klinefelter’s syndrome is genetic and can be considered a form of being intersex. It occurs when a boy has more than one X chromosome, leading to lower androgen levels and higher estrogen levels. This increased amount of estrogen can increase the risk factor.
Can trans men get breast cancer?
Anyone can get breast cancer. However, transgender men and non-binary people occupy a unique space regarding risk factors and following the breast cancer story from start to finish. Many AFAB (assigned female at birth) men or non-binary people carry the same risk factors that cisgender (non-transgender) women have, especially if they have not taken steps such as gender-affirming surgery or hormone therapy.
Most data on the subject of transgender and non-binary people and their risk and experience with breast cancer comes from individual case studies and anecdotal experiences rather than extensive cancer research. One such study conducted in 2013 in the Netherlands examined nearly 800 AFAB trans men taking testosterone and discovered only one case of breast cancer. Overall, the study stated that “The rate of breast cancer among trans men in this study was estimated to be much lower than the rate of breast cancer among cisgender women and similar to the rate among cisgender men in the Dutch population” (1).
Do top surgery or binding affect breast cancer risk?
Binding, a practice not uncommon among trans men and non-binary people, compresses the breast tissue to make the chest seem flatter to help reflect the person’s gender identity more accurately and comfortably. Binding can sometimes cause adverse symptoms such as shortness of breath, pain, and skin infections, especially when done by more risky methods (tape, ace bandages, leaving binders on for too long). However, binding has not been linked to breast cancer.
Top surgery, a mastectomy performed to align the patient’s breasts and chest with their gender identity, is a different form of mastectomy from those performed for breast cancer purposes. Top surgery mastectomies remove fatty tissue but may leave behind some glandular (milk-producing) tissue and lymph vessels, where cancer may form. People who receive top surgery should still perform regular breast self-checks and discuss the risks of cancer with their doctor.
Can male breast cancer kill you?
There is a risk of death as with any cancer, depending on when the breast cancer cells are discovered. According to the American Cancer Society, the prognosis for breast cancer in men is similar to that in women. The odds of surviving five or more years after the initial diagnosis are, on average:
96%–when cancer is still only affecting the breast tissue at diagnosis
83%–when cancer has spread through the breast to nearby areas, such has the local lymph system (underarm, etc.)
23%–when the disease has spread throughout the body
Just as is recommended to women, it is essential to be aware of any changes in the breast so that if cancer cells start to grow, treatment can begin as soon as possible.
What is the survival rate of male breast cancer?
As mentioned above, 2,550 new cases of breast cancer in men are diagnosed annually. Unfortunately, this same cancer also leads to around 480 deaths in men. While this is significantly lower than the close-to-40,000 women who die of breast cancer annually, it is still a statistic that can be lowered.
Most male breast cancers are diagnosed after patients discover a lump in their chest. However, many tend to leave this concern alone until other, more severe, symptoms arise, such as blood coming from the nipple. However, by this time, the cancer has likely spread further, making the necessary treatment harsher and the risks involved a little grimmer.
By informing male patients of the possible risk factors for breast cancer, they can be more aware should they notice something out of place in their chest. Self-breast checks can be just as necessary for men, transgender, and non-binary people as for cisgender women, and everyone should have the chance to be informed of their risk.
If you have questions about your risk factors, any changes in your breasts, or simply about breast cancer, speak with your doctor, or Dr. Gorman at the Texas Breast Center is happy to help answer any questions. Her goal is to keep all patients informed and prepared.
Gooren LJ, van Trotsenburg MA, Giltay EJ, van Diest PJ. Breast cancer development in transsexual subjects receiving cross-sex hormone treatment. J Sex Med. 2013;10:3129-34.
Breast cancer is a vicious disease that is far more prevalent than we would like. One in eight women will receive a breast cancer diagnosis in their life, and one in one thousand men receive the same. However, more rarely discussed when mentioning these statistics is the risk of breast cancer for transgender people.
Transgender people–those who identify with a different gender than the one they were assigned at birth–may choose to receive treatments to align their bodies with the physical standard of their gender. This process, called transitioning, can include surgeries as well as gender-affirming hormone therapy. While some find these changes unnecessary, others rely on them to feel comfortable in their own bodies.
What gender is most likely to get breast cancer?
Most people could tell you that women are more likely to get breast cancer than men. And while this is correct, many don’t know the reasons why. Between the excess breast tissue and ‘female’ hormones, the female gender identity seems to come with risk. This includes both cisgender–those who are not transgender–and transgender women. However, everyone of any gender should invest in regular breast checks, looking for lumps or any other possible changes to their breasts.
Risk for Trans Women
An increased amount of estrogen and progesterone, commonly known as the female hormones, in the body for any reason will increase the breast cancer risk for anyone, regardless of gender. However, these two hormones can both be used in hormone treatment for trans women or non-binary people, giving their bodies access to more than they naturally produce. While this is perfect for helping transition (alter their physical characteristics to match their gender identity) it does introduce an increased risk where there wasn’t as high a risk before.
Risk for Trans Men
Transgender men, however, tend to lower breast cancer risk factors through both surgical means and cross-sex hormone treatment. Trans men and some non-binary people receive top surgery, a form of mastectomy that removes the breasts to give them flatter chests. While this procedure is different from a mastectomy performed to clear out breast cancer, a large amount of breast tissue is still removed. With less breast tissue, there is, simply put, less room to develop breast cancer. However, the lymph nodes and glandular tissue–two places breast cancer is likely to form–are usually still left in place. Also, consider that scars left behind can make breast imaging for breast cancer screening difficult.
Furthermore, breast cancer cases in trans men are relatively low because of their own hormone therapy. Trans men, and some non-binary people, go through testosterone therapy. Testosterone, commonly considered the male hormone, can bring trans men’s physical appearance closer to that of the general male population. And, while an unusually high amount of androgens–hormones relevant to sexual development, including testosterone–can lead to an increased breast cancer risk, testosterone treatment doesn’t tend to add enough of the hormone to the body to cause this kind of higher breast cancer risk.
Cisgender People
When discussing cisgender people, breast cancer development is far more likely to happen in women. However, even among cisgender women, some are more at risk than others, especially due to factors out of their control. For example, those who started menstruating early and became menopausal late have an increased risk. This increase is due to the excess amount of estrogen and progesterone these women were exposed to; as with trans women, the excessive amount increases the risk of breast cancer.
Cisgender men generally have the lowest risk of breast cancer. However, this does not mean they have no risk. Cis men absolutely should still be aware of the signs and symptoms of breast cancer, such as breast pain and nipple discharge, as well as the risk factors, such as family history and testicular surgery.
Is Trans hormone therapy dangerous?
As with any medical procedure or treatment, there are some risks to hormone treatment. Taking estrogen while smoking, for example, increases the risk of blood clots. One risk of taking testosterone is a high hematocrit count, or overly thick blood, leading to a possible stroke or heart attack. And while many trans men, trans women, and non-binary people may choose not to pursue hormone therapy due to these risks, one must also consider that those listed above are not the only people who utilize this treatment.
Many cisgender menopausal and postmenopausal women participate in hormone replacement therapy to treat their menopausal symptoms. The boost in estrogen that they no longer naturally produce minimizes their hot flashes and vaginal discomfort and has even been proved to reduce bone fracture and prevent bone loss.
Risks for this treatment are commonly listed as blood clots, stroke, heart disease, and, of course, breast cancer. So, while it is well known that hormone treatment alters the absolute risk of breast cancer, this is not strictly an issue for transgender people.
Who has the highest risk of breast cancer?
A Dutch study published online in 2019–”Breast cancer risk in transgender people receiving hormone treatment: nationwide cohort study in the Netherlands“–investigated the risk of breast cancer in transgender people receiving hormone treatment between 1972 and 2016 from a specialist clinic in Amsterdam (1). In this time, 2,260 trans women and 1,229 trans men were treated. In the population of transgender women–those assigned male at birth (amab) but identify with the female sex–15 cases of invasive breast cancer were diagnosed, approximately .7%. However, among cisgender women, the statistic is closer to 12.5% or one in eight women.
Of the transgender men–those who were assigned female at birth (afab) but have a male gender identity–examined in the study, only four cases of invasive breast cancer were diagnosed. This gives trans men a standard risk of approximately .3% if the study is trusted. Cisgender men receive breast cancer diagnoses in one in 1000 men, approximately .1%. However, the numbers and data pulled from the study are not the be all end all for transgender breast cancer risk statistics. More research needs to be done to have more confidence in the numbers.
However, using the data we have available from the study, those with the highest risk of breast cancer are the general female population, with cisgender women having the highest risk of all. Trans women follow after, then the general male population, with cisgender males having the lowest risk of breast cancer.
It is crucial for transgender people to understand the health risks that can come with transitioning. While many choose not to transition, many consider it of absolute importance to their health, both physical and mental. Further research needs to be done to better understand just what transitioning means to understand any potential side effects or health problems. Patients will need to know their new risks and new preventative measures to perform that they may not be familiar with, such as regular self-breast checks.
Dr. Gorman at the Texas Breast Center works to keep her patients informed of breast cancer risks, screening options, and treatment. Each patient she and her team see is treated with a personalized and targeted treatment plan.
March is Women’s History Month. The history of women and the history of breast cancer go hand in hand. But how far back does the history of breast cancer go? How long have we known about it, and how long have we been able to treat it? This article will discuss treatments and diagnoses of breast cancer since antiquity.
Who first discovered breast cancer?
When did breast cancer start?
Breast cancer, and cancer as a whole, has likely been around as long as humanity has. Evidence of prostate cancer has been found on skeletons of both a Russian king (approximately 2,700 years old) and an Egyptian mummy (about 2,200 years old). But the earliest record we have of breast cancer can be found on the Edwin Smith Surgical Papyrus, an Egyptian papyrus dating back to 3000-2500 BC. While the papyrus does not offer much in the way of treatment options, it does give a way to identify an incurable disease as “cool to touch, bulging and spread all over the breast.”
Ancient Greece, around 460 BC, gave us the term carcinoma (karkinoma). Carcinoma is a cancer that starts in skin or organ tissue cells rather than in structures like blood vessels or bones. However, breast cancer treatment was still relatively unsuccessful as it was believed that disease was caused by imbalances of the four humours, phlegm, yellow bile, black bile, and blood. To treat illnesses, one had to remove or increase the humours within the body. Galen, a well-known Greek physician from around 168 BC, claimed that breast cancer was caused by too much black bile and began to treat the condition with surgery to remove the tumor, though he let the incisions bleed to continue removing excess bile.
While the surgery that Galen performed spread throughout Greece, the increase in religious philosophies and medical approaches prevented the practice from going much further. Early Christianity believed surgery to be more barbaric than their faith healing preference, a tradition that persisted through much of the world between 476 and 1500 AD. However, between the 10th and 15th centuries, Abu Al-Qasim Al-Zahrawl and Ibn Sina, a pair of Islamic physicians, revived the Greek practices, including surgery, and wrote many medical texts. Their ideas and practices spread throughout Europe.
The 16th, 17th, and 18th centuries, known more commonly as the Renaissance period, saw a growth in surgical practice. Where once ‘surgeon’ was simply a title tagged onto the end of ‘barber’, and a procedure could be performed after a haircut, surgeons now had their own trade. John Hunter, a Scottish surgeon, proposes the first idea of breast cancer in stages. While not as clearly defined as those we have today, there were some stages where surgery was necessary, while others were not. This was also a time of no anesthesia, so these early lumpectomies and mastectomies had to be performed quickly and accurately.
As the 19th century rolled around, significant improvements were made to the safety of surgery. With the introduction of hygiene to medical practices (albeit slowly), disinfection and surgical garments became more common. Anesthesia was also developed, helping prevent patient shock and give the doctors more time to perform the breast cancer surgery. William Halsted, an American surgeon, developed the radical mastectomy procedure in 1894. This procedure removes the entire tumor in a single piece together with the breast, the axillary lymph nodes, lymphatic vessels, and pectoral muscles. This was the first time breast cancer was considered treatable and even curable. Two years later, Thomas Beatson, a British surgeon, announces that oophorectomies–operations to remove one or both ovaries– can reduce tumors in advance breast cancer.
Modern Breast Cancer Treatments
The 20th century brought vast change to breast cancer treatment. Tumors were shrunk using radiation. Chemotherapy was introduced in the 1940s, and Robert Egan introduced mammography as a breast cancer detection option in 1962. The first modern autologous breast reconstruction was performed in 1979, allowing for more natural feeling breasts. More medications, procedures, and treatments for breast cancer have been researched and implemented, as well as potential causes and risk factors. The BRCA1 and BRCA2 genes–commonly known as the breast cancer gene– were discovered in 1995. A few years later, new breast cancer subtypes–HER2 positive, triple-negative, progesterone receptor-positive, and estrogen receptor-positive–were classified in 2000.
Even today, new research is still being performed to improve upon the surgeries, treatments, and post-op for breast cancer patients to have the best possible results. Dr. Gorman was involved in a study using the Biozorb implantable marker that helps target radiation therapy as well as post-operation imaging. She also contributes to the study on Accelerated Partial Breast Irradiation, or APBI, a method that shortens the amount of time the patient needs to spend getting radiation therapy and uses a higher dose of radiation in a more targeted beam–assisted by the Biozorb marker. She also uses oncoplastic techniques which help with postoperative cosmesis.
Breast Cancer Treatment Today
With today’s understanding of the disease, treatment is far more effective than it has been in the past. One primary reason for this is the improved breast cancer screening guidelines and understanding of breast cancer risk factors such as family history or having the so-called ‘breast cancer genes’. Knowledge of these risk factors can help set up specific screening procedures for those with a higher risk of breast cancer while still having a standard screening arrangement for those with lower risk. Getting a regular mammogram and breast self exam are easy steps to keep an eye out for early potential signs and symptoms. The sooner breast cancer is caught, the easier it is to treat.
Once a breast cancer diagnosis is reached, a treatment plan is agreed upon; no patient’s treatment plan and recovery are exactly alike. Treatment plans can–but do not necessarily–include breast surgery, radiation therapy, chemotherapy, hormone therapy, targeted medical therapy, as well as cosmetic surgery to aid in the patient’s self-image after an oncological procedure. Each of these treatment options has benefits and downsides and side effects and is more useful in some situations than others. The different surgical approaches can be applied depending on the tumor’s size and how far the breast cancer cells have spread. There are options to save more of the breast tissue and chest muscles if the breast cancer is caught early enough.
Combination treatments–surgery accompanied by radiation therapy or chemotherapy alongside medical therapy, for example–can help by approaching the breast cancer from different angles, ensuring thorough results with no cancer cells left behind and decreasing recurrence. With a combined effort from a full oncological team, the survival and recovery rates have increased exponentially since the days of the Edwin Smith Surgical Papyrus.
Dr. Gorman and her team at the Texas Breast Center work together to treat breast cancer from all angles. Dr. Gorman focuses on treating from the surgical side and works closely with medical and radiation oncologists to form a personalized treatment plan best suited to each patient. She also looks to the future of treatment by keeping aware of current and ongoing breast cancer research to best treat her patients. If you have questions or are ready to find your next steps in treatment, reach out to the Texas Breast Center. The team is prepared to help.
An essential part of breast cancer awareness and breast cancer prevention is breast cancer screening. Screening takes many forms, from the self-breast check to the breast MRI, but all play their part. These screening examinations provide an opportunity to catch signs and symptoms of breast cancer, as well as lumps, early so that treatment options can be less extreme. Here is some information on the basics of different tests, when and how they are taken, and the decision-making process behind them.
When should I start breast cancer screening?
While any person with breasts should start a regular breast self-exam as their breasts start to develop, clinical screening does not need to begin so early. Different organizations vary in their breast cancer screening recommendations, especially as it comes to when exactly you should begin your breast cancer screening. Your particular risk and family history can play a part in your timeline.
When should I get screened for breast cancer?
The general timeline recommends:
Ages 25-39: Self breast exam monthly; annual clinical breast exam; mammogram for high-risk patients (annually, starting 10 years before youngest family member diagnosed with breast cancer)
Ages 40-54: At age 40, patients with normal risk start annual screening mammogram.
Ages 55+: It is recommended that screening continues for as long as the patient is still living a healthy life and is expected to do so for at least ten more years. According to the U.S. Department of Health and Human Services, women between 40-74 with screened mammograms have a decreased chance of dying from breast cancer.
As with any medical concerns or tests, ask your doctor the best time to start your breast cancer screening and how often you should go.
What are the screening tests for breast cancer?
There are a handful of different kinds of breast cancer screening tests, each with its own purpose and use, as well as benefits and risks.
What are Clinical Breast Exams?
A clinical breast exam is an exam performed in a doctor’s office by a doctor or other health professional. They will use their hands to feel and check for any physical abnormalities, signs, or symptoms of breast cancer in the breast and surrounding areas. These include lumps, irritated or puckered skin, and swelling.
The doctor will also ask for any relevant information such pregnancy history or the date of the patient’s last period. These can affect a patient’s risk of developing breast cancer and the current state of their breast. It is always best to be familiar with your own breasts look and feel so you can note any changes to your doctor straight away.
Most often, when a woman finds a lump or other sign or symptom, it tends to be during dressing, bathing, or other regular activities. However, doing these regular physical and visual checks, especially self-checks, keeps you familiar with your breasts’ regular state, so you are more likely to notice a change.
What is a mammogram?
A mammogram is the most common method of breast cancer screening in women ages 25 and above. It is a low dose x-ray exam that provides internal images of the breast. Mammography is an integral part of early detection because it can find small changes within the breast before these changes can be felt or seen by the patient or their doctor. Ductal Carcinoma in Situ (DCIS) can also be found early in mammograms. DCIS is a collection of abnormal and/or pre-cancerous cells in the milk ducts of the breasts. The sooner breast cancer is found and treated, the better, as it is usually much easier to treat in early stages.
As with any medical test, there are some risks. Because it is an x-ray, there is radiation involved. However, it is such a low dose, and such a brief exposure, that no radiation is left in the body after the examination. These risks also include the chance of a false-positive in the test results. A false positive can be caused by particularly dense breast tissue, scar tissue, or other factors. However, most doctors will not give a positive diagnosis purely based on just the mammogram due to the risk of false positives. They will recommend another form of test to compare results. There is also a 10-15% risk of a false-negative test result from a mammogram.
Another form of this test is digital mammography, also known as 3D mammography or tomosynthesis, which is particularly helpful for women with dense breast tissue or other factors that might cause a false positive on a typical mammogram. This screening exam can improve the chances of finding small cancers while reducing the need for additional testing to confirm false positives. 3D mammography does give a clearer picture of the breast tissue.
Other Breast Cancer Screening Tests
A few other types of breast cancer screening tests are used less commonly, though each has its purpose. These screening tests are generally used for women or patients with many risk factors, such as a family history of breast cancer or a genetic predisposition for breast cancer, or potential positives in previous mammograms.
Breast MRI Screening–MRI, or Magnetic Resonance Imaging, uses radio waves and magnets to collect detailed images of the body. This is often used for high-risk patients and those with a genetic mutation that increases their risk of breast cancer. This may actually start prior to mammogram on these high-risk patients.
Breast Ultrasound–An ultrasound of the breast can be used when a woman cannot undergo an MRI or x-ray screening (for example, if they are pregnant). Ultrasounds are particularly useful on dense breast tissue, containing more glands or ducts than fat. The ultrasound can differentiate the dense tissue and breast cancers better than traditional mammography. If there is no contraindication, however, a patient also needs a mammogram.
Thermography– Thermography uses a heat-sensing camera to observe and record the temperature of the breast’s skin. Because some tumors cause temperature changes, the thermogram may detect the presence of these tumors. However, there have not yet been any randomized clinical trials of this test to determine its validity. This may be additional information for your physician but does not replace annual mammograms.
What is the most accurate test for breast cancer?
Each test used to screen for breast cancer, from the breast self-exam to the breast ultrasound, has benefits and risks. Mammography is the easiest screening test to access and has been found to to find DCIS and other breast cancer tumors reliably, and is best for average-risk women. However, 5-15% of mammograms need a follow-up by another test for clarification. Ultrasounds can add diagnostic information on a painting and can help give a clearer picture than a mammogram, especially for women with dense breasts. MRIs are also helpful diagnostic tools for women with dense breasts and can sometimes find cancers that were even missed by the ultrasound. MRI cannot be used by those who have metal implants or are allergic to the contrast.
Each of these types of cancer screening exams works uniquely to collect different results. Ask your doctor for their recommendation based on your personal risk factors and concerns.
Does screening for breast cancer really work?
No one breast cancer screening exam is going to find 100% of breast cancer. However, between regular screening and breast self-checks, the chance to find breast cancer while it is still in the early stages increases dramatically. The sooner breast cancer can be detected, the easier it is to treat, and therefore the easier treatment will be on the cancer patients.
Remember, you can speak to your doctor or healthcare provider about your risk factors and determine your best method and pacing for screening. Dr. Gorman and her team at the Texas Breast Center are always happy to speak with you about breast cancer and any next steps in treatment plans.
A breast cancer diagnosis can seemingly come out of nowhere for many patients. However, many things that could have made this diagnosis (or any potential diagnosis) far more likely for some patients than others. These little details in lives are known as risk factors. Some factors are a part of your lifestyle and can be controlled in your day to day life. Others are beyond a given person’s control, like things built into the DNA. It’s important to note that none of these factors will cause breast cancer. Any one of these risk factors is not a cause for breast cancer. They will only bring about higher risk.
Risk Factors You Can Affect
Taking hormones–Some forms of hormone replacement therapy (HRT), including estrogen and progesterone, in menopause can increase the breast cancer risk.
Using oral contraceptives–Some birth control pills have been found to raise breast cancer risk.
Reproductive history–A few factors relating to childbirth can vary your risk level. Having your first pregnancy after the age of 30, not having children, never having a full-term pregnancy, or not breastfeeding can increasing your breast cancer risk.
Being physically active–Women who are more active will decrease their risk of getting breast cancer.
Being overweight after menopause–Older women with obesity have an increased risk as opposed to those at a healthier weight.
Alcohol–The more alcohol someone drinks, the higher the risk of breast cancer. For example, a woman who has 2-3 alcoholic drinks a day will have a 20% higher risk than a woman who does not drink.
Diet–There is some debate about what diets increase or decrease the risk of breast cancer. However, a healthy diet with plenty of fruits and vegetables and minimizing animal fats has many health benefits.
Smoking–Smoking can increase a person’s risk of breast cancer.
Night shift/light at night–Routinely working night shifts can bring about a higher risk of breast cancer, possibly due to light exposure at night.
Risk Factors You Cannot Affect
Sex–A woman is far more likely to get breast cancer than a man due to the increased exposure to estrogen and progesterone. Because these are the hormones used in hormone replacement therapy for transgender women, this increased risk includes them. While men can certainly get breast cancer, the risk is not as high.
Race–White and black women are most likely to develop breast cancer. Black women tend to have the highest risk before 45 and are more likely to die from the disease.
Ashkenazi Jewish heritage–Jewish women also have a higher risk of breast cancer, likely due to a high occurrence of the BRCA1 and BRCA2 gene mutations in those of Ashkenazi Jewish descent.
Inherited genes–Several genes that can act as risk factors for breast cancer.
BRCA1 and BRCA2
ATM
BARD1
BRIP1
CDH1
CHEK2
NBN
NF1
PALB2
PTEN
RAD51C and RAD51D
STK11
TP53
Age–As you get older, your risk of breast cancer increases. Most diagnoses occur after the age of 50, and by the time a person is 60, the risk of breast cancer is 1 in 29. Breast History–If someone has previously been diagnosed with breast cancer or another breast disease like lobular carcinoma in situ or atypical hyperplasia, they have a much higher risk of breast cancer in the future.
Family History–Women who have a family history of breast cancer, especially when it is a first-degree relative (mother, sister, daughter) previously diagnosed. The risk of breast cancer also increases with multiple family members diagnosed, and a family history of ovarian cancer can also indicate an increased risk.
Radiation Exposure–Previous exposure to ionizing radiation in the chest area is a risk factor for breast cancer. Radiation is often used for treating Hodgkin’s disease. The risk is greater if the radiation was applied as a child.
Age at First Period–Starting menstruation early, before ages 11 or 12, can raise the breast cancer risk factor by bout 15-20% over those who started to get their periods at 15 or older. This is due to more prolonged exposure to estrogen and progesterone, which, as mentioned above, increases risk.
Age Starting Menopause–Women who start menopause after 55 have an increased risk of breast cancer by approximately 40% compared to those who start at age 45 or younger. Like with the earlier start of menstruation, this is due to more prolonged exposure to progesterone and estrogen.
Breast Density–Breast density comes from having more connective tissue than fatty tissue. This denser tissue can make it very difficult to read a mammogram accurately, sometimes increasing the risk of missing a potential diagnosis. Breast density can come from high estrogen levels, indicative of a risk factor rather than one on its own.
History of Diethylstilbestrol (DES)–DES was a drug given to some pregnant woman between the 1940s-1950s to prevent miscarriage. Those women and those whose mothers took it all have a high risk of breast cancer.
Birth Weight–Women born with a higher birth weight have an increased risk of breast cancer, particularly before menopause.
Blood Androgen–Androgens are hormones important to sexual development (including testosterone). An increased amount of androgens in a woman’s blood can increase her breast cancer risk.
Bone Density–High bone density can be a breast cancer risk factor. Someone with high bone density can have up to 60-80% higher risk than those with lower density.
For a deeper look at Breast Cancer Risks, read our Causes series, starting with this article on Family History Risks.
Reducing Risk
Breast Cancer Screening–Go for regular breast screening to keep an eye on your breast health. For most, a mammogram is sufficient for checking breast health. A Breast MRI (Magnetic Resonance Imaging) may be better for those of higher risk. Speak with your doctor to establish the best course of action for the frequency and type of screening for you.
Breast Self-Exam–Monthly, you should check your own breast health. While it won’t necessarily catch every sign of breast cancer, it can find many, and it is an excellent way to keep yourself familiar with your breasts. By checking your breasts’ appearance, feel, and textures regularly, you will be more likely to notice any changes should they come. If anything does change, bring it to the attention of your doctor.
Breast Feeding–Breastfeeding can help reduce the risk of breast cancer, particularly in those pre-menopause.
Lifestyle Changes–As mentioned above, some breast cancer risk factors that can be reduced through your own lifestyle choices. By doing what you can to handle these risk factors, such as alcohol intake and physical activity, one can reduce their risk of breast cancer by a great deal while also keeping themself healthy in general.
Speak With Your Doctor
If you are ever concerned about your risk of breast cancer, you can speak with your doctor. While some risk factors are easy to determine for yourself, some must be tested for–blood androgen levels, inherited genes, etc.–which your doctor can help you get access to and understand. Once you and your doctor are familiar with your breast cancer risk level, you can set up a plan for your next steps. These will include recommendations for breast cancer screening–how often and what type–as well as possible medical preventative steps if your risk of breast cancer is high enough.
Dr. Gorman at Texas Breast Cancer is always available to help with any questions about breast cancer risk, preventative steps, and the process should a breast cancer diagnosis be given. She is an advocate for the informed patient, always providing her patients and those who could potentially become patients with the information they need.
If you have any questions about breast cancer or breast cancer risk factors, please feel free to contact Dr. Gorman or her team at Texas Breast Cancer.
When breast cancer comes backs, it is called recurrence. While those who have a recurrence are not in the majority, they are certainly not a rarity or an impossibility. Recurrences typically happen within the first five years after treatment but can occur at any time and have a few ways of returning. To help ease some of the worries of these first few cancer-free years, we want to give some clarity and explanation into what breast cancer recurrence is and what to look for.
Breast cancer recurrence occurs when cells from your original breast cancer manage to escape being treated and begin growing again. This process can sometimes take years. The cancer cells will lay dormant until something kick starts them into growing again.
Risks
Many of the recurrence risk factors are determined by the original tumor and cancer, though the patient determines some. These risk factors include:
A large tumor–A larger tumor increases the risk of cells being left behind.
Close or positive tumor margins–During surgery, when the surgeon removes the cancer, they will remove a small amount of healthy tissue around it. The tissue is then examined with a microscope. If it is clear of cancer, the margin is considered negative. However, if there are any cells left (considered a positive margin), risk or recurrence increases.
Lymph node infection–The risk of recurrence increases if cancer was found in lymph nodes at your original diagnosis.
No radiation treatment post-surgery–While most who undergo a lumpectomy choose to receive radiation therapy in the area of cancer afterward to reduce the risk of recurrence, some do not.
Inflammatory breast cancer–This type of breast cancer increases the risk of a local recurrence.
Specific cancer cell characteristics–Having triple-negative breast cancer or cancer resistant to hormone therapy can increase your risk.
No endocrine therapy–For certain types of breast cancer, not receiving endocrine therapy can raise the risk of recurrence in cancer patients.
Younger age–Those of a younger age during their initial breast cancer diagnosis, specifically under 35, have a higher risk of their cancer returning, despite generally older generally being a risk factor of cancer in general.
Obesity–Increased body mass index increases the risk of breast cancer coming back.
Prevention
There are methods and steps you can take to reduce your risk of recurrence of breast cancer, many in your initial treatment.
Chemotherapy–Those with an increased chance of recurrent breast cancer have been shown to have a decreased risk when treated with chemo.
Hormone therapy–If you have receptor-positive breast cancer, taking hormone therapy in your initial treatment can reduce your risk. This treatment method can sometimes continue for five or more years.
Targeted therapy–If your cancer produced additional HER2 proteins, targeted drug and treatment might reduce your risk.
Radiation therapy–A previous breast cancer patient with a large tumor, a breast-sparing operation, or inflammatory cancer would have reduced risk if treated with radiation treatment.
Bone-Building–Bone building medications can reduce the risk of recurrence taking place in bones, otherwise known as bone metastasis, for those with a high risk.
Healthy Diet–To decrease your risk of breast cancer recurrence, be sure to include plenty of fruits, vegetables, and whole grains in your diet, as well as limiting alcohol to one drink a day.
Exercising–Exercising regularly may help reduce your risk.
Kinds of Recurrence
Recurrent breast cancer can take one of three forms, defined by where it appears in reference to the primary cancer and treatment. The three types are local, regional, and distant recurrence.
Local
A local recurrence occurs when cancer cells grow in the same area as your previous cancer. If a lumpectomy was used for treatment (rather than a full mastectomy), cancer might start to regrow in the breast tissue that remains. If a complete mastectomy were performed, the tissue along the skin or chest wall would hold the recurring breast cancer.
Some signs that local recurrence is occurring are:
One or more painless lumps, nodules, or irregular areas of firmness under the skin
Newly thickened areas along mastectomy scars
Changes to the skin (inflammation, redness, changes in texture)
Nipple discharge
Many of the signs of a local recurrence are similar to those of initial breast cancer. After treatment, it does not hurt and may help to continue self-breast exams to keep an eye out for any changes, just in case.
Regional
Regional recurrence also happens rather close to the original site of infection. However, the difference between regional and local recurrence is a matter of lymph nodes. In regional recurrence, the local lymph nodes, such as those under the arm, will be infected with cancer.
Signs of regional recurrence cancer may include a lump or swelling in lymph nodes, so continue your self-checks in these areas:
Under the arm
Along the neck
Near and in the groove above the collarbone
This kind of recurrent breast cancer can almost be considered a subset of local recurrence and can many times be found by being familiar with your own body. Regular self-breast checks are just as necessary after breast cancer treatments as they are before.
Distant
Distant recurrence is when cancer recurred somewhere in the body away from the original site. This can include other organs such as the lungs or even bones. In this case, the patient is generally treated much in the same way as those diagnosed with stage IV breast cancer. However, treatment can vary from standard stage IV treatment based on the responses to previous treatments.
Treatment
Treatment, many times, is determined by the kind of breast cancer recurrence found. Local will be treated differently from regional will be treated differently from different.
Local Treatment
Local breast cancer recurrence is, if possible, treated with surgical treatment. If a lumpectomy and radiation were used previously, then a mastectomy would be the first choice treatment. If a mastectomy was performed prior, the tumor would be removed, and the patient will be treated with radiation therapy if not already received.
Either way, both of these plans are likely to be accompanied by chemotherapy, targeted therapy, hormone therapy, or some combination to ensure a full recovery.
Regional Treatment
Sometimes breast cancer will come back in the lymph nodes. This can be treated by removing the lymph nodes themselves, followed by radiation in the surrounding area, if not already received. Systemic (targeted, hormone, or chemotherapy) treatment after surgery may be discussed on a case-by-case basis to ensure that any remaining cancer cells are eliminated.
Distant Treatment
The primary treatment for distant recurrent breast cancer will be a form of system treatment (hormone, targeted, or chemotherapy) based on how your cancer has responded before. You and your doctor can create a treatment plan that serves you well, knowing what has worked with these breast cancer cells previously and what has not.
Dr. Gorman
Dr. Valerie Gorman and the Texas Breast Center are aware of the risks of recurrent breast cancer and the chances that your breast cancer may come back. This is why she and her team stay with you through your personalized treatment and long after to make sure you know that you always have a support system, whether you need it or not.
Dr. Gorman specializes in surgical oncology and surgical diseases of the breast. She serves as the Medical Director of Surgical Services at Baylor Scott & White Medical Center as well as the Chief of Surgery.
After a mammogram, some women find out they have dense breasts. They come to me with questions about what that means, how it affects their risk for breast cancer, and what they should do differently. Here’s how I answer the questions I hear most often.
What does it mean to have dense breasts?
It’s common for women to have dense breasts. Your breasts are made of fatty tissue, which is not dense, and supportive tissue, milk glands, and milk ducts, which is. The parts of your breast made up of dense tissue show up as white on a mammogram, so it can be harder to spot signs of breast cancer in those areas.
How do I know if I have dense breasts?
The radiologist who reviews your mammogram assigns a grade to your breast density based on how much of your breast tissue is dense. You might see something on your mammogram report called Breast Imaging Reporting and Data System (BI-RADS). There are four levels of breast density:
A is almost all fatty tissue, found in about 10 percent of women
B is more nondense than dense, found in about 40 percent of women
C is more dense than nondense, found in about 40 percent of women
D is almost all dense, found in about 10 percent of women
If you fall into the C or D categories, your mammogram report may indicate that you have dense breasts. If it doesn’t say, ask your doctor.
As you can see, about half of all women have dense breasts. You’re more likely to have dense breasts if you are younger, have less body fat, and/or take hormone therapy for menopause.
How does my breast density affect my risk for breast cancer?
Since it’s harder to spot breast cancer on dense breasts, you have a higher chance of cancer not being detected on a mammogram. Separately from that, women with dense breasts also have a higher risk of breast cancer.
What should I do differently if I have dense breasts?
You should talk to your doctor about your other risk factors for breast cancer and work together to come up with a breast cancer screening schedule that works for you. For my patients with dense breasts but no additional risk for breast cancer, I recommend an annual mammogram beginning at age 40. Depending on other risk factors for breast cancer, I might also recommend:
A breast MRI, which uses magnetic forces to image your breast
A 3D mammogram, which combines images of your breast taken from different angles
Breast ultrasound, which uses sound waves to investigate areas of your breast that might be concerning
Molecular breast imaging, which uses a radioactive tracer to look for cancerous areas
While most people are familiar with the idea and repercussions of breast cancer, not everyone may know what exactly breast cancer is or how it comes to be.
Kinds of Breast Cancer
Put simply, breast cancer is the continued growth of abnormal cells in the area of the breast. This area can include the ducts (that carry milk), lobules (that produce milk), and connective tissue (that holds everything together. Most breast cancers start in the lobules or ducts. And while this does mean cancers appear in the area that we traditionally think of as the breast, it includes the underarms as well.
But there is not one single type of breast cancer. And sometimes, the types overlap.
Invasive Ductal Carcinoma
With invasive ductal carcinoma, cancer cells start in ducts and spread out into the surrounding breast tissue. If it continues to spread to other parts of the body, it metastasizes.
Invasive Lobular Carcinoma
Invasive lobular carcinoma starts in the lobules and spreads to nearby breast tissue. This cancer can also metastasize.
Less Common Types
There are many other kinds of breast cancers, though most are less common. Medullary breast carcinoma starts similarly to invasive ductal, but grows slowly and only rarely spreads to the lymph nodes.
Mucinous or colloid carcinoma is a variation on invasive ductal carcinoma. However, the cancer cells float in mucin, an ingredient in the body’s natural mucus.
Paget’s Disease of the nipple originates with cancer cells collecting in and around the nipple, traditionally the ducts there. From there, it can spread to the areola and further.
Inflammatory breast cancer is also a variation on invasive ductal carcinoma. It is generally accompanied by symptoms of inflammation such as swelling, dimpling, and redness.
Triple-Negative breast cancer does not have the three common receptors found in breast cancers. These receptors are for estrogen, progesterone, and HER2 (human epidermal growth factor). Without the receptors, some methods of treatment are not available.
Ductal carcinoma in situ, or DCIS, is considered either the earliest stage of breast cancer or pre-cancer that is likely to lead to breast cancer. Cancerous cells are forming in the ductal lining, but they have not spread.
How Breast Cancer Spreads
Breast cancer cells start in ducts, lobules, and breast tissue. However, they can spread to the lymph nodes, raising the odds of metastasis–cancer cells spreading through the lymph system and the rest of the body. The more lymph nodes that have cancer cells, the more likely metastasis is. However, metastasis is not an inevitability. Some people with cancer cells in their lymph nodes do not have metastases. And, unfortunately, metastasis can occur despite there currently being no cancer cells in the lymph nodes.
What Are Breast Cancer Symptoms?
There are several possible changes to the breast that can be noticed in regular–monthly is recommended–self-breast checks. Keep an eye out for any changes to your regular breast shape, texture, or color. Some changes that may indicate the need to visit a doctor are:
A lump in the breast or armpit
Swelling or change in size to any part of the breast.
Discharge of any kind that is not milk coming from the nipple (including blood)
Puckering of the nipple/Inversion of the nipple
Flaky skin or redness around the nipple or the breast
Dimpling of the skin (like the skin of an orange) on the breast
Pain in any part of the breast
Any one of the symptoms on its own does not mean you have breast cancer. They could indicate an infection or changes due to hormonal shifts. However, if the signs continue or you are concerned, bring them to the attention of your doctor.
Risk Factors
There is no one sign that someone will or won’t get breast cancer, but there are some risk factors that can raise your chances. Some of these factors are genetic factors, while others come from a person’s lifestyle.
Some of the factors that cannot be reduced are:
Gender–being a woman increases your risk
Age–risk increase with age
Dense breasts–they are harder to see through on a mammogram, making early detection more difficult
Family history–the risk is increased if a close family relative (mother, sister, daughter) has had breast cancer
Personal history–previous breast conditions or breast cancer increase risk
Certain gene mutations–BRCA1 and BRCA2, as well as other mutations, can increase risk
Radiation exposure–while this may come from many sources, even medical treatment, it could potentially be a risk factor.
Starting your period young
Starting menopause older
Can Risk be Reduced?
Some potential risk factors come from lifestyle practices and can be adjusted for. Some of these factors are:
Alcohol–drinking in excess can increase risk
Obesity–obesity can increase your risk, particularly after menopause
Taking hormones–certain forms of hormone replacement therapy (progesterone and estrogen, primarily) can increase risk when taken for over five years after menopause. Some birth control pills can also increase breast cancer risk
Not having children or having them at an older age can increase risk.
Excercise–by not exercising, breast cancer risk can increase. Maintaining a healthy exercise schedule for yourself, you can lower your risk.
Prevention
The best way to prevent breast cancer in yourself is to maintain the risk factors that you can. Beyond that, keep yourself familiar with your breasts with a monthly breast self-check. More than anything, this keeps you familiar with the size, texture, and sensation of your breast so that you might be more likely to notice a change should one appear.
Also, speak with your doctor about breast cancer screening. They know the best time to start screening and will help you to the next steps if there are any concerns. Checking in on your breasts yourself, having your doctor check, and having regular screenings will help you be prepared and catch anything early should there be any signs of breast cancer to find.
Dr. Gorman
Valerie J. Gorman, MD, FACS, works to ensure that her patients are informed and receive a personalized approach to cancer treatment and breast cancer surgery. If you have questions about breast cancer or how it is treated, she or the team at Texas Breast Center in Waxahachie are happy to help answer your questions.
Dr. Gorman is board certified by the American Board of Surgery and serves as Medical Director of Surgical Services and Chief of Surgery at Baylor Scott & White Medical Center – Waxahachie.
The FDA, or U.S. Food and Drug Administration has recently approved two new medications for breast cancer treatments. The approval for these treatments was expedited due to the COVID-19 pandemic. One of these medications targets metastatic triple-negative breast cancer, while the other targets HER2-positive cancers.
Richard Pazdur, the director of the FDA’s Oncology Center for Excellence, stated, “As part of FDA’s ongoing and aggressive commitment to address the novel coronavirus pandemic, we continue to keep a strong focus on patients with cancer who constitute a vulnerable population at risk of contracting the disease. At this critical time, we continue to expedite oncology product development.”
FDA Approval
The drug’s applications were granted by the FDA under the provision known as “accelerated approval” due to today’s current conditions. This means that the drugs may be distributed and administered under specific criteria. There will still be further data from further clinical trials required before full approval is granted.
The medications may be administered to patients only when certain conditions are met. For Todelvy, this means that it is “reasonably likely to predict a clinical benefit to patients” who have are in serious condition and have unmet medical needs. For Tukysa, the medication must be administered alongside chemotherapy, and there must be at least one prior attempt at treatment.
Trodelvy
Trodelvy, also known as sacituzumab govitecan, is one of the medications to receive accelerated approval. Produced by Immunomedics, Trodelvy received approval based on results from a clinical trial (phase 1/2) of 108 patients. These patients had all received at least two treatments previously for their metastatic cancer.
It was given intravenously. It is formed of a combination of SN-38 (a metabolite of irinotecan, a chemo drug) and a monoclonal antibody that targets an antigen that induces cancer cell growth. The response rate in breast cancer patients in the trial was 33%, and 55.6% of those responders maintained their response at least six months.
Some common side effects of Trodelvy are nausea, fatigue, anemia, low white blood cell counts, as well as hair loss, rash, and abdominal pain. There are chances of more severe side effects to keep an eye out for, such as severe diarrhea and neutropenia–an abnormally low level of neutrophils.
Tukysa
Tukysa is the brand name of tucatinib, a tyrosine kinase inhibitor of HER2 proteins. When taken with capecitabine and trastuzumab in adult patients, it is intended for advanced metastatic, HER2-positive breast cancer, including brain metastases. The patients must have attempted at least one anti-HER2-based treatment geared towards metastasis.
This medication has been shown to inhibit the phosphorylation of both HER2 and HER3 in-vitro, or in lab studies. Further clinical trials will be performed.
Some common side effects of Tukysa are fatigue, liver problems, decreased appetite, hand-foot syndrome, and mouth sores, as well as others. The liver problems can become more severe, as can diarrhea, leading to other health problems.
Breast Cancer Treatment
Many adjustments have had to be made in day-to-day life with the introduction of the Novel Coronavirus. This includes the treatment of breast cancer, the testing of medication, and FDA processes of approval. These new medications have been pushed forward into the market more speedily than usual, but that does not mean they were pushed forward recklessly.
Each was pushed forward by the Food and Drug Administration with certain conditions to met before application. Each must also continue testing before the FDA approves it fully.
A recent study by the researchers at Loma Linda University Health has discovered a link between dairy milk and an increased risk of breast cancer. The study called Dairy, soy, and risk of breast cancer: those confounded milks was published to the International Journal of Epidemiology.
The study used a participation group of 52,795 North American women with a mean age of 57.1 years who were all free of breast cancer. The study then followed them for nearly eight years, taking into account their diets, demographics, family history, and other factors. A food frequency questionnaire, or FFQ, was used to estimate the women’s dietary intake. In contrast, a baseline questionnaire covered the other factors, including physical activity, hormonal and other medication use, alcohol consumption, reproductive and gynecological history, and breast cancer screening.
How much dairy milk?
At the end of the study period, the participation group yielded 1,057 new breast cancer cases. Using the FFQ, the study revealed that there is “fairly strong evidence that either dairy milk or some other factor closely related to drinking dairy milk is a cause of breast cancer in women,” according to Gary E. Fraser, MBChB, Ph.D., first author of the paper. He continued, “Consuming as little as 1/4 to 1/3 cup of dairy milk per day was associated with an increased risk of breast cancer of 30%. By drinking up to one cup per day, the associated risk went up to 50%, and for those drinking two to three cups per day, the risk increased further to 70% to 80%.”
While the particular fat content of the dairy milk–skim versus whole, etc.–had a minimal variation, when compared to minimal or no milk intake, high consumption of dairy milk and dairy calories were associated with a higher risk of breast cancer. Cheese and yogurt yielded no critical associations.
However, there was no clear association found between soy products and breast cancer. Fraser noted that “the data predicted a marked reduction in risk associated with substituting soy milk for dairy milk. This raises the possibility that dairy-alternate milks may be the optimal choice.”
One suggested reason for the link between dairy milk and breast cancer is the sex hormone content of dairy milk. Because cows are lactating when their milk is collected, approximately 75% of a dairy herd is usually pregnant. Breast cancer in women is hormone-responsive. Therefore, taking in this additional level of hormones could cause a higher blood level of it, and then insulin-like growth factor-1, which is thought to increase the risk of breast cancer, as well as other cancers.
Does Dairy Cause Cancer?
Does dairy cause cancer? There is certainly no proof of that being the case. But now there is some evidence of a link between dairy and breast cancer. “This work suggests the urgent need for further research,” Fraser said. “Dairy milk does have some positive nutritional qualities, but these need to be balanced against other possible, less helpful effects.
Risks
It is, however, worth remembering that just because an association was found does not imply causation. The numbers are just strong enough to keep researchers watching the intake of dairy, even when other factors were removed. And while Fraser stated that, “By drinking up to one cup per day, the associated risk went up to 50 percent, and for those drinking two to three cups per day, the risk increased further to 70 to 80 percent,” even that does not mean you are increasing your risk to 50% or 80% by drinking milk.
The 50% increased risk of breast cancer is a 50% increase to your current risk. If the average woman has a 1/8 chance of being diagnosed with breast cancer, that gives her approximately a 12% chance to increase the risk of breast cancer by 50% would only bring her risk up to a total of 18%. The 80% increased risk of drinking milk products 2-3 times a day would bring the total risk up to 21.6% risk of breast cancer. And while that certainly isn’t the happiest number to think about, it is certainly not as frightening as a jump to 80% risk would be.
Fraser and the rest of the researchers who worked on the study advise taking a look at current dietary guidelines, taking this increased risk of breast cancer with dairy intake into account.
If you have any questions about your risk, or possible next steps, Dr. Gorman and the Texas Breast Center are happy to help.
Dr. Gorman and the Texas Breast Center are still taking patients, but understand that there is hesitance in this time of COVID-19. To help ease fears and discomfort for patients, we have implemented certain safety measures, following Baylor Scott & White’s COVID-19 Safe Care Plan.
In-Office Policies
While some things have changed in the processes for patients and visitors to the Texas Breast Center, we are back to a full schedule. To maximize our patients’ safety, we are offering virtual care via video conferencing with your doctor for some appointments. There is also a drive-thru option for specimen collection. The waiting room is currently closed according to the Centers for Disease Control and Prevention guidelines, so when a patient arrives, they will wait in their car until an exam room is ready. When they are informed a room is ready, they will be escorted directly to their rooms. To encourage social distancing for both the patient and physician, only one visitor will be allowed to accompany the patient back. Everyone must wear a mask, including patients, visitors, and medical team members.
There will also be a screening process upon entry checking for any temperatures above 99.6 F as well as asking about potential COVID-19 symptoms such as cough, shortness of breath, sore throat, or others. If the patient answers yes to the questions or has a fever, they will be quickly moved to a separate, designated area, to prevent the spread of infection. If a visitor has a fever or answers, yes, health services will be offered. If the visitor does not need them at that time, we will request that they return home and contact their primary care doctor.
Policies and procedures are a little different when it comes to surgery rather than a general appointment or checkup at the facility.
Pre-Surgery Policies
While a surgeon’s preparatory efforts start happening well in advance of the surgery, usually a patient does not need to take any action until the day before. However, under the Safe Care guidelines, patients have a few tasks they must take care of in the week leading up to their surgery to assist in potential disease control.
Each patient is enrolled in a digital care journal five days in advance to help monitor them for fever or other symptoms of COVID-19. This online journal also offers resources to each patient who has questions. Then, 48 hours before the procedure, each patient will be tested, even if not symptomatic. Many people infected with COVID-19 are asymptomatic and can spread the virus without being aware of the risk. This is why both the testing and the personal journal are essential to your treatment. The results will determine how you and your medical team members proceed from there.
If your test comes back negative, you do not have the virus. You will not be called with the results if this is the case and can proceed with your surgery as expected. However, be aware that if the test is taken within the first 1-2 days after being infected, the results may show negative. So processes are in place at the hospital to keep patients safe, including masks worn by all hospital staff. If the COVID-19 test reveals a positive result, you have an active infection. In this case, you will be called by a healthcare team member to give you information on how to care for yourself and protect those around you. We will notify the local health department of your positive test–we are required to do so–so that you do not have to worry about it. Your surgeon and team will make a case-by-case determination on whether to postpone your procedure or continue as scheduled based on specific health needs and requirements.
When surgery takes place, all patients and visitors are screened upon entry to the building. On the day of the procedure, each patient is allowed one visitor, and then one for every 24 hours they remain admitted.
Personal Health and Safety
The Centers for Disease Control and Prevention has given us many guidelines and pointed us in a direction to follow to best care for our patients. In following these guidelines and setting up some ourselves to keep our patients safe, we have implemented new options and arrangements. As stated above, virtual care and telemedicine options are now available before and after procedures and surgeries whenever appropriate so that patients may stay home and away from hospitals.
Along these lines, Virtual Waiting Rooms have been implemented. These are patient portals used to communicate updates about care, scheduling, etc. between the hospitals, doctors’ offices, and surgery centers. These ‘waiting rooms’ can be used to set up messaging via text or phone calls as well so that there is the absolute minimum time spent in common areas.
Everyone within the buildings, including staff, patients, and visitors, must be masked and participate in social distancing to assist each other in minimizing the spread of COVID-19. We have also implemented touch-free protocols, involving paperless registration, and enhanced cleaning protocols, including UV-light disinfection.
Dr. Gorman
Dr. Gorman understands that for our breast cancer patients, the COVID-19 pandemic is only increasing the stress and anxiety in an already challenging and uncertain time. However, with the Safe Care plan, we are doing everything we can to help our patients navigate and continue on their journey to recovery.
The week of December 10, Dr. Valerie Gorman attended the annual San Antonio Breast Cancer Symposium to give a poster presentation for her research in 5-day SBRT radiation. This symposium is an opportunity for those involved in breast cancer research to share what they have learned.
The SABCS’ stated objective states that the conference “is designed to provide state-of-the-art information on the experimental biology, etiology, prevention, diagnosis, and therapy of breast cancer and premalignant breast disease, to an international audience of academic and private physicians and researchers.” Research is brought from all of these categories to be shared and help other practitioners improve their own research or treatments.
Dr. Gorman praises this conference for the multidisciplinary spread of study. As her breast cancer team is interdisciplinary, she can gather information that will interest every member of her team. She noted that there were presentations this year on “molecular studies on circulating tumor cells, more targeted therapies, and many other topics. Together with our oncology colleagues and team members, we’re able to use these to treat our patients in a collaborative, multidisciplinary fashion.”
For example, while Dr. Gorman does not specialize or perform chemotherapy treatment, she took note of several tailored researched studies into chemotherapy. There is new research being done on HER2 positive cancer, or breast cancer that tests positive for human epidermal growth factor receptor 2. HER2 protein excess is found in approximately 20% of breast cancers, caused by a gene mutation in the cancer cells. There is also chemotherapy targeting metastatic breast cancer, which is cancer that has spread beyond the point of origin–in this case, the breast and lymph nodes nearby. Patients with these cancers tend to have a lot of, and many kinds of chemo throughout their treatment. These new studies are helping us to learn how to “study the tumor and retailor the chemotherapy to the individual patient and their needs.”
The presentation that Dr. Gorman and her team were most interested in, however, came from the University of Florence in Italy. They presented on the ten-year results of breast cancer patients who had been treated with Accelerated Partial Breast Irradiation (APBI), a treatment Dr. Gorman has been using and perfecting for many years.
The use of radiation therapy on breast cancer is a common occurrence. This treatment directs high energy rays directly at the cancerous area to kill any cancerous cells left over after surgery. Traditionally, radiation therapy is implemented over 30 days. This regimen includes visits every weekday for six weeks and can potentially lead to burns on the surrounding tissue as well as changes in the patient’s appearance. However, APBI shortens the number of days needed for the treatment. Some protocols of APBI give radiotherapy twice a day for five days, while others–including Dr. Gorman’s practice–only give it once a day for five days. While the treatment itself takes little time in office, doctors know transport and waiting room time can take up valuable time from the patient’s personal and work life. By minimizing how many office visits are required, these doctors are giving their patients more of their life back.
The presentation that the University of Florence gave reveals new results from patients ten years after their surgeries and radiotherapy treatments. The results found that survival rates at the ten-year mark for those who received APBI–as with the five-year mark–matched the survival rate of those who received longer treatments. However, APBI has better cosmetic results and less burn damage.
Dr. Gorman is pleased to know that this treatment helps her patients, not only by treating their breast cancer but also by lessening the impact that breast cancer has on their personal life. With few in-office treatments, there is less time away from the office or the family. The APBI also produces more favorable cosmetic results, which can help with a healthier mindset as you approach healing.
Dr. Gorman and her team offer APBI when necessary to provide the breast results and the least interference in her patients’ lives. They also provides necessary breast cancer surgery to best help a given case. As the Chief of Surgery and Medical Director of Surgical Service of Baylor Scott and White Medical Center in Waxahachie, Dr. Valerie Gorman, MD, FACS is ready to answer your questions and design a personalized cancer treatment plan for you.
Dr. Valerie Gorman, MD, FACS, is a breast cancer surgeon, board-certified by the American Board of Surgery. She specializes in surgical diseases of the breast and surgical oncology, serving as the Chief of Surgery and Medical Director of Surgical Services at Baylor Scott & White Medical Center in Waxahachie, Texas.
As she helps her patients through the process of learning their best options for cancer treatment and the most effective type of surgery to help, her staff works with her. But she also knows that she is not the last step in the healing process. It is common for breast surgery for cancer to require reconstruction. So Dr. Gorman has an established partnership with Dr. Potter that has now lasted more than 15 years.
Dr. Jason Potter, MD, DDS, is a plastic surgeon who serves the greater Dallas area and has affiliations with multiple hospitals and hospital systems. He is double board-certified, with his advanced surgical training focusing on reconstructive plastic surgery. He serves the greater Dallas area.
The Breast Reconstruction Interview
Dr. Gorman and Dr. Potter recently sat down for an in-depth interview on breast reconstruction surgery.
Dr. Gorman and Dr. Potter’s partnership is based on mutual respect for both each other and the patient. The two sat down in a joint interview to explain how their collaboration worked and how it benefitted the patient.
Here are some highlights of the interview.
To start, Dr. Gorman was asked why she chose to work with Dr. Potter. She answered,
“We both have the same standard for our patients. He doesn’t do the easy way; he does the right thing for the patient. He can offer every option to our patients, so he’s not just limited to one kind of breast reconstruction. I think other plastic surgeons recommend what they do. And he does it all, so it makes it easy to recommend the best thing for each patient.”
Breast Reconstruction Options
Dr. Potter explained his reconstruction options:
“The two main types of reconstruction are either implant-based reconstruction or tissue-based reconstruction. Patients are not always a candidate for both. Sometimes there are limitations put on us by the patient’s body habitus, such as how much tissue they have to donate for breast reconstruction or prior surgeries that prevent utilizing tissue from certain areas. So most of the time, implants will always be available, but if patients have had multiple infections or have a history of radiation, there are higher complication rates for implant surgery.
However, some people don’t want an implant. They’ve never had an implant, and they never will have an implant. They just don’t want one. Implants require maintenance. You have a new device in the breast that has to be maintained, has to be monitored, and has to be replaced approximately every ten years. Whereas, when you have an all-tissue breast reconstruction, the patient doesn’t necessarily need other surgeries once they’ve completed the process because maintenance isn’t required. It’s really sitting down with the patient, seeing what co-morbidities or preferences they might have or bring to the table, and then selecting the best option.”
Factors Taken into Account for Reconstruction
Several factors have to be taken into account when figuring the best approach to breast reconstruction. Dr. Gorman usually starts the process when discussing the initial breast cancer treatment.
Dr. Gorman:
“Usually, the patient is in my office first, so I try to get a good understanding of them, and I try to learn a little about what the patient would like to do. I usually have an idea of when he would like to offer somebody one or the other, considering the patient’s preference, their medical situation, their questions, and what they already know. I then go from there. Some factors I look for are if they’re a smoker, or if I see they’ve had several abdominal surgeries. If they’ve had radiation before, I know we’re going to have to do a flap to try to protect that implant, those kinds of things. I leave it open for Dr. Potter to use his expertise and talk to them about the pros and cons of each option available.
Some people don’t want a massive surgery. The flap is a longer, second operation, so many people want to avoid that. But in the long run, 20 years from now, that 8 hours in the operating room, they’re not going to remember that part. So, we try to talk them through what they want and what we think they’re tending to prefer and talk about the pros and cons. If they’re a smoker, there may be certain options that have reduced risk. Then we send them to Dr. Potter, and he finishes the conversation, and they make the final decision. And our offices coordinate scheduling whatever procedure we’ve decided together with the patient.”
Dr. Potter added:
“It’s a nice team approach. From the day they go into Dr. Gorman’s office, they’re starting to get questions answered; they begin to have reconstruction questions answered. As soon as they find out they’re going to need a mastectomy, they want to know what that next step will be. Dr. Gorman is very good at starting that discussion with them. After surgery, both offices work with the patients when they have issues in the postoperative period, so it’s a nice comprehensive approach to patient care. I think the patients really like it.”
The Breast Reconstruction Process
Once the patients have met their doctors, the process can begin.
Dr. Potter:
“Breast reconstruction is a process, so it’s not usually one operation and done. It starts the day of the mastectomy with either placement of a tissue expander (which is a temporary implant) or initial reconstruction using the patient’s own tissue in certain situations. But operations are usually staged about three months apart. So, if surgery was all the patient needed, they may complete reconstruction in six months or so. If they need chemotherapy or if they need radiation, they may not complete the reconstruction process for nine to twelve months. It’s kind of hard to say exactly how quickly they can have their surgery, but they’re staged depending on the procedure and patient’s needs and other treatments.”
Dr. Gorman said about the stages:
“A lot of people come in and say, ‘I want it all done in one operation,’ which we can sometimes do. But we talk to the patient about how sometimes that’s not the best solution for them because they’re going to end up having another operation down the road anyway. So, whether it’s one stage or two-stage, we tend to go with two-stage for improved cosmetic outcomes. Once again, those are just the different options we offer.
The DIEP Flap Procedure
Another variation of the reconstruction options mentioned above is whether the DIEP flaps procedure is being performed. Dr. Potter is well known for his ability to perform this operation.
“Not everyone does the flaps. That’s a big operation, and Dr. Potter does a significantly high volume of these. He’s the DIEP flaps guy. If you mention DIEP flaps to anybody, his name comes up. We offer that to our patients, which is awesome.”
Dr. Potter gave a little more detail into the DIEP procedure, saying:
“It’s a complex reconstructive procedure. Not every surgeon offers these techniques. Because of its complexity, patients are better served by an experienced team like ours. For the last 13 years, we’ve been providing that operation in Dallas. We have a very efficient team, which is important for patients so that they’re not under anesthesia too long. We’re also refining the technique and leading some of the advances. We are are now providing Resensate™ to candidate patients. Resensate is a technique to provide reinnervation to the breast.”
Reinnervation is the restoration of nerves to a place where there has been nerve damage, like a surgical site. This has been a concern of plastic surgeons for as long as this has been a profession. To explain the importance of Resensate and its work in reinnervation, as well as patient expectations, Dr. Gorman explained,
“The biggest thing when you’re educating patients about breast reconstruction after they get a mastectomy is that they’ll say, ‘oh well, my friend had implants, so this is kind of like that, at least I get a breast augmentation and implants like my friend did.’ And then you have to remind them, ‘your friend kept her breast, and yes, she has the same implants in there, but it’s very different.’ And the sensation is the most significant difference there probably. The way they feel and look are different, too, but the sensation is very different. And we have heard a wide variety of comments from patients who have had this procedure, from ‘they feel like they are floating in front of me,’ to ‘I have some intermittent feeling, it comes back over months,’ to somewhere in between. I think that’s the most significant difference, once they get over the initial surgery and diagnosis and treatment. Settling back into everyday life, it is a constant reminder. It is hard to forget what they’ve been through because it is so different. So gaining feeling back will be huge because it is one of the big reminders for them.”
Common Questions About Breast Reconstruction
Now that there is a general understanding of the types of breast reconstruction and the process of moving between the breast cancer surgeon to the plastic surgeon, Dr. Potter discussed some of the common questions he gets asked at appointments.
“There are lots of questions about tissue-based operations versus implant-based operations. There are lots of questions about the types of implants given, and the recent Allergen textured surface recall. And really, the most common question is ‘which operation is best for me? We try to take patients through that question because that discussion is never the same for any two patients. Recovery is always a concern. Most questions here deal with downtime, recovery, time off work, and number of surgeries.
Recovery varies with the operation and the patient. With the first operation–the mastectomy and the tissue expander–it can be anywhere from 2-4 weeks of downtime. Implant surgeries are usually less downtime for the first stage, and tissue surgeries can be up to 6-8 weeks, depending on what they choose.”
The recent concerns about textured implants have resulted in many questions regarding implant safety. He continued,
“Overall, implants are very safe. A recently identified process called Breast Implant-Associated Anaplastic Large Cell Lymphoma has brought renewed scrutiny to breast implants. Allergen was asked to voluntarily recall their textured surface implant line because 80% of the cases found worldwide were associated with that implant surface. But it’s an extremely rare process.
Despite its rare occurrence, many patients going through breast cancer treatment do not want to worry about other potential problems linked to the reconstruction. This is leading more patients to inquire about tissue-based options.”
In summary, whether receiving a tissue or implant breast reconstructive surgery, Drs. Potter and Gorman know to listen to you, to listen to each other, and work with the best materials to ensure the best outcome for you.
Final Thoughts on a Team Approach to Breast Reconstruction
When asked for their final thoughts, Dr. Gorman had this to say,
“The team we’ve formed between our offices and the options we offer together are what I want to emphasize. Between the two of us, we can more thoroughly follow-up. If a patient goes to see him, he will ask me any questions that need asking. If they need to have drains removed but don’t want to drive all the way to him, they can stop in our office to get them taken out. We do a lot of that for the patient, which I think is pretty great for them. We navigate them through the post-breast reconstruction hassle. We can say ‘yes, we’ve talked to them, you’re good to go here or do this’ so they don’t have to go back and forth between us and say ‘well Dr. Gorman said this’ then they say ‘well Dr. Potter said to let you know that.’ This way, the patient doesn’t have to do all that on their own.”
Dr. Potter followed up in agreement.
“It is a very personal, very comprehensive approach. Patients are going to appreciate the individualized attention that they are going to get every step of the way. And the way our offices work together, it helps to coordinate and make sure the patient doesn’t have to determine which office to go to.”
Drs. Potter and Gorman work cohesively to ensure their patients are receiving the best care. By staying in contact, there is no risk of loss of information. By working with each other consistently, they learn how the other works and can better inform patients on what to expect. Dr. Potter’s expertise in types of breast reconstruction and Dr. Gorman’s cancer-oriented breast surgery go hand in hand to create a strong team approach for treatment, recovery, and your best outcome.
Last month was breast cancer awareness month, a time to highlight the importance of cancer screening and breast health. The Center for Disease Control has named breast cancer as the most common cancer for women in the United States. Approximately 12% (that is, 1 in every eight women) will be diagnosed with invasive breast cancer over her lifetime.
These statistics shift depending on other factors like age, race, and certain genetic factors. For example, African-American women are far more likely to be diagnosed with triple-negative breast cancer than women of other races, and to die of breast cancer of any kind. Asian, Native American, and Hispanic women tend to have lower risks of developing breast cancer, though they should still be aware of the signs and symptoms.
Why is Breast Cancer Screening Important?
In September of 2019, the American Cancer Society announced a new stance on breast self-exams. They stated that self-checks do not tend to reveal any early signs of cancer when women are also getting their scheduled breast cancer screening mammograms and regular checks by their health professionals. That’s not to say that people do not come to their doctors after spotting changes in their breasts. However, these changes are often noticed during dressing or bathing.
Despite this announcement, breast checks can still provide valuable insight. It is easiest to spot changes in your breast if you are familiar with it in the first place. If you are doing a regular breast self-exam, you will be ready to catch anything out of the ordinary–whether that be during your exam or while getting dressed.
How to do a Breast Self-Exam
There are two basic steps to a breast check. You’ll want to examine the breasts by looking and by feeling. Both of these steps can be further broken down from there. Try to do all parts of the exam on the same day and around the same time in your cycle every time: a week after your period ends is a standard time to do it. If you don’t get a period, set a date every month to do your breast self-exam.
Look
For the looking portion of the check, you will want to stand in front of a mirror. You will be standing in a few different poses and looking at a few different angles–front, right, and left.
In each of your poses, you will want to look at a few factors. Make a note of the shape of your breasts, especially in comparison to one another. It is far from unusual for one to be larger than the other, but sudden or drastic changes in size should not happen. Keep an eye out for a change in the usual vein patterns in your breasts. If the veins have increased or expanded significantly, you may want to speak with your doctor. Symptoms display in your nipples if they are consistently itchy, red, swollen, scaly, inverted, or are producing discharge. Finally, check the skin on your breasts for dimpling, redness, rash, puckering, or anything that could be considered like an orange peel. These could all be signs of something happening beneath the surface.
The best way to look for all of these symptoms is to examine your breasts from all angles. First, face the mirror with your arms down at your sides. Turn to the left and the right to check both sides of each breast. Next, place your hands on your hips with your elbows out to your sides, keeping your shoulders up and back. Repeat the pattern of front, left, and right. This same pose can be done hunched forward. This adjustment allows the breasts to hang so that you can see the underside.
Now, raise your arms straight above your head. You can clasp them together or leave them in a superman pose, but try to remember what you have done in previous breast exams so that you know what to expect. Once you have made a thorough observation, lean forward at the hips so that your breast hang forward again, keeping your arms above your head.
Make a note of anything you find that is different from normal and keep an eye on it. Many symptoms we attribute to breast cancer can also be symptoms of things like PMS, a swollen lymph node due to another infection, or many other factors, though, so observe first. However, if you have strong concerns, don’t hesitate to call your health professional for answers.
Feel
To start the feeling check, you will want a comfortable and flat place to lie down. You will lay flat on your back with your right arm up behind your head (if you are starting with your right breast). The goal is to get your breasts as flat as possible.
Once you are in a comfortable position, you will want to start feeling along the outer edge of your breast, near your armpit. You will want to use the pads of your fingers rather than your fingertips and move in small, smooth circles. Perform each circle at more than one pressure–light, medium, and firm–between the size of a dime and a quarter. By varying the amount of pressure, you can check more of the breast tissue. Move in a slow, up and down pattern across until you have covered the entire breast. Another option is to start at the nipple and perform your press checks in a spiral outwards. So long as you have a pattern to ensure you cover the entire breast and become familiar with it, this should be sufficient. Try to follow the same pattern every time you do your breast self-exam.
Once you have finished your exam lying down, it is best to give your breasts an exam while standing or sitting up as well. You will use the same pattern you have established for yourself, using firm, medium, and light pressure and the pads of your fingers to feel for anything unusual in the breast tissue you might have missed while lying down.
When is a Breast Lump Cancer?
It’s not entirely uncommon to find some kind of lump or bump when doing your breast self-exam. Hormones, infections, and other causes can cause temporary lumps that you may detect during your monthly checks. There are common attributes that a cancerous lump will have, though none are a guarantee. If you are concerned about anything you find, have your doctor examine it as well.
Your fingers can detect the most common criteria for a cancerous lump during your breast self-exam. The lump will be a firm, painless mass. The edges are sometimes irregular. If you have a lump that is getting larger over time, that may also be a cause for concern.
Of course, each case is unique. Some cancerous lumps may be painful or soft, and some may feel perfectly round. They can be more challenging to detect in people with more dense breast tissue or scar tissue on their breast–for example, those who have had previous breast surgery. These denser tissues can also make it somewhat more difficult for mammograms to detect cancer. People with dense breast tissue or scar tissue should be particularly familiar with their breasts so that they can detect changes early.
What Causes Breast Cancer?
While there is no one singular cause of breast cancer, there are several risk factors that could increase the likelihood of a diagnosis. Some are environmental factors that may be controlled, while others are physical characteristics or part of your history.
Gender, race, age, and genetics are all potential risk factors. Women are more likely to develop breast cancer, and this risk increases once they reach the age of 55. Some genes, like the BRCA1 and the BRCA2 genes, can be passed through generations and are considered a potential cause. If a first-degree relative (a daughter, sister, or mother) has or had breast cancer, your risk doubles. Because of the importance of hormones as a risk factor, your menstrual history may also be a factor. Those who started their period early–before the age of twelve–may have an increased risk.
Some risk factors are situational or environmental. Tobacco and alcohol use can increase your risk, especially in younger patients, as can being overweight or obese. Some previous benign or noncancerous breast conditions may influence your risk later on. Hormone use, such as hormone replacement therapy, both current and in the past, can increase your risk. One risk factor that is easier to lower is living a sedentary. Exercising regularly will decrease your risk of developing breast cancer.
Breast Self-Exam Results
The primary purpose of a breast self-exam is to help you to familiarize yourself with your breasts. If you know what the skin, muscle, and tissue feel like on a typical day, then you will be better prepared to notice anything abnormal should something come up.
These tests are not a reason to avoid getting a mammogram or having a physician examine you, especially if you are among those with risk factors. If you do come across something in one of your breast self-exams that has you concerned, bring it up with your doctor, or with Dr. Gorman at the Texas Breast Center. As a surgeon specializing in surgical oncology and surgical diseases in the breast, she can help you understand whether your lump, change in skin texture, or any change is a cause for concern. And, if it is, she and her team will help you set up a treatment plan.
Valerie J. Gorman, MD, FACS, is board certified by the American Board of Surgery and serves as Chief of Surgery and Medical Director of Surgical Services at Baylor Scott & White Medical Center – Waxahachie. Her goal is to ensure that all of her patients have an informed, personalized approach to breast surgery and cancer treatment.
Breast cancer and accompanying treatment can be a grueling experience, both physically and emotionally. And while relief can come with successful surgery, recovery can difficult. Here is some information about what to expect from recovery and a few tips to make it easier.
Your Hospital Stay
After surgery, you will stay in the hospital for the first steps of recovery. How much time you spend in the hospital differs depending on the type of surgery, whether it was outpatient or inpatient, whether reconstruction was performed, and other factors.
A lumpectomy is traditionally an outpatient procedure. It does not require an extended stay in the hospital—less than 23 hours—as the stay is merely to give the surgeon and nurses enough time to make sure there are no adverse aftereffects. Once they are satisfied, you may leave the hospital to better rest and fully recover.
A mastectomy, however, can require an extended stay. When lymph nodes are removed, and breast reconstruction is performed, you may have to stay in the hospital 1-2 days. Without the reconstruction, this may drop to overnight, though this is still considered an inpatient procedure. More complex reconstruction may require a longer stay. Always ask your doctor how long they expect you will have to stay before you can leave the hospital.
Anesthesia
Anesthesia keeps a patient unconscious, painless, and calm during surgery and is carefully catered to each patient’s needs. Medications can be changed due to an individual’s allergies or previous experiences. Anesthesiologists will also adapt their medicines depending on the procedure. For example, general anesthesia is commonly used for these procedures.
General anesthesia can, in a small number of people, cause adverse reactions and symptoms. A sore throat can come from the tube placed in the throat to help with breathing during the procedure. Nausea, vomiting, delirium, itching, chills, and muscle aches are common side effects. Some may be caused by accompanying pain medication, but each sensation should pass rather quickly.
Pain After Breast Cancer Surgery
As with any surgery, some level of pain should be expected after breast surgery. Initially, this will come from the surgery itself, based around the incision sites and where the tissue was removed. If lymph nodes were removed, there would likely be more pain. As healing begins, the pain will settle more when you are still and be triggered more by a range of motion. As the breast, breast tissue, lymph nodes, and underlying muscles are so central to the body, almost any movement of the body can affect this area. Your surgeon will inject local anesthetic during surgery to reduce post-operation pain.
To help control pain levels, your surgeons will prescribe medication that will drop off into over-the-counter medicines that will drop off into no medication when you are ready. When the pain is still severe, you may be placed on something like tramadol for the early days. You will be weaned off of these drugs and onto over the counter pain medication within the first few days to prevent complications.
Drain
When tissue is removed from a surgical site, there is a risk of seroma. Seroma is a build-up of fluid to fill in a suddenly empty space in the body–a place where there once was tissue, and now there is not. Seroma can be uncomfortable or even painful, and can sometimes scar. To prevent this issue, the surgical team will place a drain in the breast that removes any fluid that attempts to fill the healing space after a mastectomy.
After the surgery, you will be given instructions on how to care for your drains. You will be told how to empty them, what to look for in them, and when they will be removed. They will likely look like a small tube leaving–and stitched to–the breast that travels to a hand-sized bulb. This bulb will be kept in a compressed position, setting up a vacuum to pull out any fluids that should be pulled out.
The bulbs have measurement labels on their exterior so that you can easily see how much fluid has drained. You will have to keep track of these measurements as you empty, clean, and recompress the drains throughout the day. These numbers help determine how long the drain will stay in place.
Living with drains can be inconvenient until you get used to them. You must always be aware of the tubes, so they don’t catch on something. Though the bulbs tend to come with loops you can strap around your surgical bra’s straps to keep them out of the way, the tubes are still something to keep in mind. There are also belts and shirts explicitly made to hold drains and their tubes.
Bathing is also tricky with drains. While you have to wait until your doctor has said you will be alright to bathe in the first time, you should not submerge your drains, so a bath is not a good idea (for your drains or your scars). Most doctors recommend gently patting yourself clean and dry with a sponge bath.
There are a few factors that you need to pay more attention to in your drains than others. You should alert your surgeon if you start to notice signs of infection, fluid leaking around the tubing, drainage increasing, decreasing, or thickening, the bulb losing suction, bright red drainage, or if the drain falls out.
What to Wear After Surgery
One reason surgery can be intimidating is that you don’t know how you’ll look when the scars have healed, and the swelling has gone down. Even with breast reconstruction, there may be changes to your appearance. Clothing can be a touchy subject. Not only will it fit you differently, but you will be sensitive for a time as your body heals.
Bras, in particular, will be difficult. Surgical bras are given and recommended in some situations, which offer some support while putting minimal pressure on incisions. They clasp in the front to avoid instigating the pain that comes from moving too much. A nurse can help adjust it easily while in the hospital, and it can be used to hand the drains to keep them out of the way of your arm.
In the first weeks after surgery, you’ll likely want to stick to bras or shirts like made in this way. Clasps, buttons, or ties in the fronts. Pants or skirts that can be easily stepped into. Nothing overly complicated or that has to be pulled over the head. This will pull on the arm and shoulder, and therefore the sensitive muscles beneath the breast. Advice commonly given by previous patients of breast cancer surgery recommend loose tops and shirts for a while. Give yourself time to adjust to your new appearance with some comfortable wear.
For the first year after surgery, bras should have no underwire. The seams should be soft, and the band should be wide to minimize any pressure on one particular place. Cups should be both full and separated. And you’ll likely want to be fitted by an expert for your new bra size. Make sure to find someone who has the training, perhaps at a lingerie shop or department store to ensure the best fit.
If you are using a breast prosthesis, you may want to find a bra with a bra pocket. These are small pockets sewn into the inside of the bra to hold a prosthetic in place. Mastectomy bras can be purchased with the pocket, or you can adapt a regular bra by sewing a pocket in yourself. Or, many find, a regular bra with a full cup that fits well enough will hold a prosthetic without a pocket. Of course, it all depends on your comfort level and what you like best.
Movement and Exercise
After breast cancer surgery–and other breast cancer treatment like radiotherapy–it can be essential to keep the affected muscles moving. Yes, they are sensitive and difficult to move. But that is precisely why you must exercise them. You don’t want them to weaken or stiffen further from disuse.
Exercise, in this case, does not mean a workout. Overworking your arms and shoulders in this condition would be easy and could be harmful. But simple exercises and movements to ensure that everything is staying in use will help in the long run. Within the first week of surgery–the first 3-7 days, if possible–you should start with the easiest movements. Use the arm on the side of the surgical site to comb your hair, practice deep breathing approximately six times a day, and raise the affected arm above the head (lay it on a pillow, so it is above) and clasp your hands open and closed 15-25 times. These are simple exercises you can do without straining too much or even getting out of bed.
Once you’ve healed more and your surgeon gives the okay, you may start other exercises. Again, these are not particularly strenuous. You are still recovering. Your muscles are not prepared to comfortably remain above your head long enough to pull a shirt on, let alone lift weights. These exercises are merely meant to keep the muscles in the area near the operation flexible. Side effects of any major surgery can be weakening of unused muscles and difficulty getting back to full strength. If you practice these minor arm exercises early, you can prevent these.
Some simple exercises can be done while sitting at your table. The Shoulder Blade Stretch is done while facing the table with your palms placed on its surface. Your back should be straight, the unaffected arm (the arm away from the surgical area) should be bent slightly. The affected arm (closest to the surgical area) should be straight. Without turning your body, slowly slide your affected arm forward until you can feel your shoulder blade moving. Relax, then slowly pull your arm back. Then you repeat 5-7 times.
If you prefer to lay down while you stretch, you can try Elbow Winging. This stretch helps the movement of the shoulders and the chest and is performed while lying on your back. It can do this stretch on a bed or the floor (whatever is most comfortable for you and your stage of healing). Once you are lying flat, bend your knees and place your feet flat on the floor. Place your hands behind your neck and clasp them together, bringing your elbows up, so they point up towards the ceiling. Carefully press your elbows out and down towards the floor. This will take a while. Your first attempt after your operation will likely not reach the floor. But as you heal, you will get closer and closer. Repeat this motion 5-7 times.
Be careful not to push yourself too soon after surgery. Wait until a surgeon has said it will be okay to exercise, so you don’t strain your wound. But remember that when you get the chance, moving is an integral part of healing.
Recovery
Recovery is unique for each person. Some feel no aftereffects from anesthesia while others hate what it does to them. Some patients’ only clothing issues come from adjusting to the surgical bra they are given immediately after surgery, while others take longer to adjust to their new appearance. Recovery is not a straight path. It is a branching and varying road from breast cancer to health. But it’s not one traveled alone.
Not only will you have your support network of family members and friends, but your medical team is there to support you as well. The surgical team will work with you to find your best procedure, find your best medications based on experience and family history, and prepare you for recovery.
Dr. Valerie Gorman knows about the concerns and fears that come with a breast cancer diagnosis. But she and her team will work with you to create the best treatment plan for your needs and lifestyle and help you find the easiest recovery path.
Dr. Gorman’s team have walked alongside many people who have been diagnosed with breast cancer and understand your situation. It is our privilege to walk with you, answer your questions, and help you through this difficult process.
In a recent survey of patients diagnosed with early-stage breast cancer, 38% said they were worried about finances due to their treatment. 14% said that their breast cancer cost them at least 10% of their household income. 17% said that they had spent even more than that 10% on out-of-pocket medical expenses.
When doctors, surgeons, and radiation oncologists were asked about how their offices handle financial discussions with their patients, 50% of medical oncologists reported that someone in their practice “often or always discusses financial burden” with their patients. 43% of radiation oncologists said they did as well. Only 16% of surgeons reported the same.
Furthermore, no one seems to know, going in, just how far a diagnosis of breast cancer is going to set them back financially. It is difficult to find answers about the cost of treatment, whether for surgery, radiation, or other medications. We are taking this chance to clear the air between doctors and patients; we can give the answers that so many have been looking for and help to start the conversation so you can be prepared should this diagnosis ever come your way.
Total Costs
In 2010, breast cancer was the highest-costing cancer in the United States. Nationwide, it cost a total of $16.5 billion. By 2020, this is expected to increase to $20.5 billion. The American Cancer Society estimates that over $180 billion is spent on health care expenses and lost productivity every year due to cancer.
How Much Does Breast Cancer Surgery Cost?
Of course, each person’s case is unique. Their access to insurance must be taken into consideration. Different stages of cancer are harder to treat than others, which can affect overall treatment costs. Not to mention that disease takes root differently in each person, so it must be treated differently. And with no one-size-fits-all treatment, there is no one-size-fits-all price tag. All of these factors must be considered.
Stages
The stage at which a patient’s breast cancer is discovered significantly affects how difficult it is to treat. A study was done recently and published in The American Health and Drug Benefits1on the cost and frequency of some treatments based on the cancer stage and how long it had been since the diagnosis.
It was not much of a surprise to find that those patients with more advanced stages of breast cancer spent more on treatments. For those with stage 0 cancer, the average cost of treatment at twelve months after diagnosis was $60, 637. After twenty-four months, the price had jumped to $71, 909 per patient overall.
For those whose cancer had advanced to stages I-II, their medical costs were approximately $82,121 in the first twelve months of treatment. In the second twelve months, each patient still in the study brought the total average to $97, 066.
With breast cancer in stage III, the average cost in the first twelve months continued to rise to $129,387. After a full twenty-four months, the study reported that patients spent an average of $159,442.
At stage IV, the most difficult to treat, the average treatment costs were $134,682 at twelve months and $182,655 at twenty-four.
According to the study, patients were paying an average of $85,772 within the first twelve months of being diagnosed with breast cancer, despite their cancer stage. And within the first two years of their diagnosis, the study reported their treatment costs averaging $103,735.
Treatments
Another major factor that will contribute to the overall cost of breast cancer treatment is the kind of treatment a patient is receiving. Which treatment you receive depends on the location, cancer stage, and extent to which the disease has spread. Sometimes the procedures are combined to get the best results and return you to health quicker and more effectively. The same study mentioned above also explored the average amount spent on categories of treatments, and how common these kinds of treatments were within the given periods.
Surgery
Surgery is a standard treatment for a breast cancer diagnosis. If applicable, it is a way to remove cancer physically from where it has taken root. Altogether, surgical treatment accounts for an average of 20% of the cost of breast cancer care treatments within the first year after diagnosis, and 4% in the second year.
Inpatient breast cancer surgery accounts for 6% of the cost treatment in the first year, and 2% in the second year. In the first year of treatment, the cost of breast cancer surgery is, on average, $4,762, while in the second year after diagnosis, the cost is approximately $347.
Outpatient breast cancer surgery accounts for approximately 14% of the price of breast cancer treatment in the first twelve months, and 2% in the second. The cost of outpatient surgery in the first and second years were found to be, on average, $11,691 and $389 respectively.
Chemotherapy
Chemotherapy is another well-known treatment of cancer. It accounts for approximately 19% of breast cancer treatment in both the first and second year after diagnosis.
For general chemotherapy, the average cost (including all costs on the day of the treatment) in the first year is $15,113. As this accounts for 18% of the payment for treatment for breast cancer, this is particularly significant. In the second year post-diagnosis, the average cost for this treatment is $3,625. This makes up 16% of all breast cancer treatment costs.
Oral chemotherapy is far less conventional. It only accounts for approximately 1% of the costs of first-year treatment, and 3% in the second year. Patients are usually paying $432 in their first year and $636 in their second year for this treatment.
Radiation
Radiation is used to kill the tumors by damaging cancer cells’ DNA. It is often used in combination with surgery. It makes up 18% of diagnosis treatment costs in the first year and 3% in the second year. In the first year, it costs an average of $15,455, while in the second year, patients pay $638.
Medication
Hand in hand with these major treatments come medications. Medications make up for 3% of the first year’s medical payments, and 7% of the second year. That equates to approximately $2,258 and $1,510, respectively.
Other Treatments
There are, of course, other treatments. Smaller subcategories that don’t quite fit these above, including hormone therapy, additional inpatient or outpatient care, or professional or specialist care. They make up about 42% of potential treatment costs in the first year and 67% of costs in the second year. That equates to $35,762 in the first twelve months and $14,980 in the second.
Health Insurance
Another factor that contributes to the overall cost of breast cancer treatment is health insurance. Healthcare, the amount of coverage you have, and the type of coverage you have, are all essential to discuss with your doctor, oncologist, and surgical team to make sure you understand where you stand.
Researchers in North Carolina found that patients who received a cancer diagnosis and did not have insurance or Medicare paid $6,711 for medication, while those with insurance paid $3,616 and those with Medicare paid $3,090 simply because they do not have the means to negotiate for a lower price.
Often, clinical appointments are more costly, as well. Where an insured patient might pay approximately $65-246, a patient without insurance coverage would pay around $129-391.
Ask Questions/Dr. Gorman
Getting a diagnosis of breast cancer is near impossible to imagine, and even harder to plan for. But if you ever find yourself in that place, you have a little more knowledge about what to expect. One should always be prepared for the unexpected, and it never hurts to have a little money saved up for emergencies. But breast cancer treatment costs will require more than just a bit of your savings. However, with communication with your team and laying out your healthcare terms and concerns as you discuss your health plan, everyone can be on the same page and do what they can to work within your needs.
Dr. Valerie Gorman knows about the financial burden that comes with breast cancer. She is dedicated to offering her patients a personalized approach to breast surgery and the treatment of breast cancer. She and her team will help to create a treatment plan that best meets your needs, and most fits your lifestyle. Because of the experience and breadth of our specialists, a multitude of treatment options exists which can be tailored to your situation.
There is no need to panic when you hear the word cancer. We have walked alongside many people who have been diagnosed and understand your fears and concerns. It is our privilege to walk with you and help you through this difficult process.
When someone is first diagnosed with breast cancer, their first concern is not often about their appearance. They might first consider prognosis. Can the surgeons get the cancer out? What are the treatment options? But if surgery is necessary, the cosmetic applications are a consideration. Your breast cancer team wants you to have the best results possible, including minimal scarring.
Breast Cancer Surgery
There is more than one way to remove tumors and cancerous cells surgically. Surgery options for the more extreme cases are the simple or total mastectomy, the radical mastectomy, and the double mastectomy. For the less severe cases are the lumpectomy or partial mastectomy, the nipple-sparing mastectomy, and the skin-sparing mastectomy. While these are still serious surgeries, these procedures can allow the patient to keep more of their natural breast shape with less dramatic scarring. While the type of procedure can certainly depend on how big the tumor or cancerous area is, treatment ultimately comes down to you, the patient, and your needs.
Breast Cancer Scars
The different variations of surgical procedures lead to different appearances, sizes, and locations for scars. With a total mastectomy, where all of the breast tissue, skin, and the nipple are removed, there will be a noticeable change in appearance. That area of the chest will be flat, and there will be a visibly large scar where the breast was.
With a skin-sparing mastectomy, the skin remains, but the nipple and breast tissue are removed. There is some room for reconstruction here under the skin, but there will still be a medium- to large-sized and prominent scar across the front of the breast.
A nipple-sparing mastectomy, however, leaves the skin and nipple and takes only the breast tissue and tumor. The scar traditionally branches off from the areola towards the armpit. It is still on the medium to large side of the scale and quite noticeable.
A lumpectomy only removes a portion of the breast tissue–that closes to the tumor–to ensure that none of the tumor is missed. This, too, can leave a large scar, which is quite visible depending on the location of the tumor and the surgeon’s approach.
All of these treatment options and their variations can be very effective with a skilled surgeon and oncology centers you are comfortable with. But they can leave a noticeable scar that many patients find a disheartening reminder:
72% of women did not realize how uncomfortable their breast cancer surgery scars would make them feel when undressed
72% of women are not displeased with the location of their scar
76% of women did not realize how uncomfortable their surgery scars would make them feel when someone else sees them undressed
82% of women have not worn a particular item of clothing because it reveals their breast cancer surgery scars
87% of women are self-conscious due to their scars
Hidden ScarTM Breast Cancer Surgery
In 2015, Invuity launched a new surgical approach to assist with just this issue. The Hidden ScarTM Breast Cancer surgery program was created to help surgeons and patients by offering less invasive methods of performing the surgery.
The Hidden Scar procedure allows for a smaller incision while still providing light in the surgical site, permitting the surgeons to treat the cancer and remove the tumor while still preserving as much of the breast’s natural shape as possible. More than that, this hidden scar process offers better cosmetic results by, as the name suggests, hiding the scars in the body’s natural folds.
Hidden Scar Mastectomy
For a nipple-sparing mastectomy, the Hidden Scar Breast Cancer Surgery scar will dramatically decrease. There can be no evidence of any cancer within the nipple for Hidden Scar Surgery, and this surgery is best suited to patients who have non-invasive cancer.
The Hidden Scar mastectomy is performed by making an incision in the inframammary fold, or the natural fold under your breast. It will naturally be hidden by the fall your breast and its small size.
Hidden Scar Lumpectomy
A Hidden Scar Lumpectomy offers options for where the incision will go, depending on where the cancer is located in the breast.
The Axilla, or under the armpit. The scar is usually hidden in a natural fold.
Around the edges of the areola. Many patients prefer this option, as the scaring is minimal and hidden even when wearing a petite bikini top.
The Inframammary fold – like the mastectomy.
Dr. Gorman and Hidden Scar
Dr. Valerie Gorman and her team have experience with the Hidden Scar approach. They have performed Hidden Scar Breast Cancer Surgery and understand the differences and options that come from each approach to oncological surgery. Dr. Gorman knows that it is important to discuss all of your options when it comes to your health and will answer any questions you may have until you can come to a conclusion with which you are happy. Contact the Texas Breast Center in Waxahachie to make an appointment and have any questions answered.
The BioZorb marker is a medical device meant to be implanted in the surgical site. Thanks to its open structure, it can be stitched into place by breast surgeons to avoid movement and allow the surrounding tissue to grow around the device after the procedure. The marker has six titanium clips that are used for future clinical imaging.
What is BioZorb Made of?
The structure itself is made of a material that is bioabsorbable, or able to be absorbed by the body. Therefore, as the tissue grows and reforms, the BioZorb can be absorbed, leaving behind only the titanium clips as tissue markers for imaging if necessary. This process takes approximately a year.
How Does BioZorb Help?
Using a BioZorb implant in breast cancer treatment can be helpful surgically, cosmetically, and with radiation treatment. Surgically, the implant–or the titanium clips if the implant has already been absorbed–can provide a perfect reference point for any future imaging for where the previous breast surgery and radiation procedures took place.
It can also assist with the structure of healing, which lends itself to improved breast cosmesis. Often with tumor removal, the breast can appear concave where the tissue grew in to fill the void the tumor left. However, BioZorb offers structure for the surrounding tissue to grow around to prevent any potential divots. This can sometimes help with oncoplastic surgery or post-lumpectomy cosmetic surgery. As for radiation therapy, the implant can provide a target for the beam to minimize the radiation damaging any surrounding tissue unnecessarily.
What are some facts about BioZorb?
Your doctor is placing an implant into your breast during this surgery. The implant is firm, but not painful and can usually be felt in the breast for 12 to 18 months, even once the surgical scars have healed. It will eventually be absorbed by the body.
When should BioZorb be used?
It is not uncommon for a patient to react strongly when they hear a diagnosis of breast cancer. They may want to avoid any risk and go straight for the total mastectomy, removing the full breast and therefore the cancer.
However, with a breast cancer team working with you on your treatment, there is more room for a personalized approach. The cancer can be treated with surgery, radiation, or a combination of the two, and when it is caught at an early stage, a total mastectomy is not needed. A lumpectomy can remove a tumor while leaving most of the breast intact.
It is in these cases that BioZorb is useful. When a patient is able to receive breast-conserving surgery, the cancerous tissue is removed by the breast surgeon, and then the skin is closed. From there, radiation may be administered by a radiation oncologist to reduce the risk of recurrence without damaging the surrounding tissue. This can be difficult without something in the breast to mark where the surgery took place. Sometimes, the empty space of the surgical site where the tumor was will fill with a liquid, forming a seroma, and this can be an indication of where to radiate.
However, if BioZorb is placed in the breast during surgery, the metal marker clips work like a road sign pointing the way for the radiologist to follow. Even after the body absorbs the coils, the clips remain in case they are needed again for imaging purposes.
Dr. Gorman and BioZorb
Dr. Valerie Gorman uses BioZorb in applicable cases to help her patients recover with less pain, less cosmetic adjustment, and more accurate imaging. But she did not take this step lightly. Before jumping all in with BioZorb, she was involved with a study testing accelerated partial breast irradiation (APBI) using her preferred intensity modulated radiation therapy (IMRT). The IMRT was directed in each of the 57 cases by a BioZorb device to keep the radiation localized.
They found that, in the follow-up visits, the cosmetic results were excellent on all accounts. Only one patient experienced pain in the area, at it was easily treated. Patients were pleased with the results.
Dr. Gorman has completed over 100 BioZorb procedures, and she and her team know the benefits it can bring. She will answer any questions you have. She always wants you to be comfortable and knowledgeable about your treatment, which is why she has done her own research into BioZorb. She wants you to receive the best treatment and best results in the long term.
If you have received a cancer diagnosis of invasive ductal carcinoma, you may not understand what that means. You may, like any of us would be, be scared. As one of the most common types of breast cancer, invasive ductal carcinoma–IDC–accounts for about 80% of all breast cancers. Also called infiltrating ductal carcinoma, cancer infiltrates and invades the breast tissue after bursting free of the milk ducts. A carcinoma is a cancer that begins in organ-lining tissue or skin. Therefore, the name–invasive ductal carcinoma–is no more than a definition of the thing it names.
What Causes Invasive Ductal Carcinoma?
Cancer can form anywhere when cells in a given area start to multiply after a change of shape or makeup. They multiply rapidly and don’t die when they should. In this case, the cells are increasing inside the milk ducts. There are several risk factors that could contribute to these changes in the cells (though sometimes the changes happen in people who do not have these risk factors and others have the risk factors and never get IDC). Some of the factors are being female, smoking, alcohol intake, previous radiation therapy, poor nutrition, family history of breast cancers, or potentially having mutations to some genes. The most commonly known breast cancer genes are BRCA1 and BRCA2 gene, which have been linked to IDC in some cases.
Is Invasive Ductal Carcinoma Dangerous?
In the early stages, IDC can be difficult to notice, as it causes few symptoms, which can make it dangerous. However, if you are doing regular self-breast checks and screening mammograms, it is likely to be caught sooner rather than later. Some signs of breast cancer to keep an eye out for during your breast checks are breast pain, nipple pain, inverted nipple, swelling of the breast (all or just a part), dimpling, irritation, redness, scaliness, or thickening of the nipple/breast skin or breast tissue, a lump in the underarm, or discharge from the nipple that is not milk.
What are the stages of Invasive Ductal Carcinoma?
Like many cancers, invasive ductal carcinoma is broken down into five stages, and each stage is measured in terms of the size of the tumor, how the lymph nodes are affected, and metastasis–where the cancer has moved throughout the body. All of these points are considered and taken into account, along with genetics, surgical results, and other considerations to assist in giving the patient their prognosis. The first stage is called stage 0, or ductal carcinoma in situ (DCIS), then Stage I is at when the cancer is starting to leave the milk ducts, and stage IV is when the cancer has spread outside the breast or auxiliary lymph nodes. For IDC specifically, this means:
Stage 0 — The disease is primarily in the ducts, though it may have spread to the lobules of the breast but no further. It is considered noninvasive at this point.
In the early part of Stage I (Stage IA), the tumor is small but has become invasive, though it still has not reached the lymph nodes. The cancerous area is between .2 mm and 20 mm.
Stage II can vary from person to person. Early Stage II (Stage IIA) can either have no tumor, but the cancer has spread to up to three lymph nodes under the arm, a 20 mm or small tumor AND have spread to the lymph nodes or have a tumor that is between 20-50 mm without any spread to the lymph nodes. Later Stage II (Stage IIB), either has a tumor between 20-50 mm and has spread to the under-the-arm lymph nodes, or it must be over 50 mm without spreading to the nodes.
Fittingly, there are three phases to Stage III. In the first (Stage IIIA), the cancer (any size) has spread to 4-9 lymph nodes–under the arm or mammary. However, it has not spread anywhere else. If this is not the case, it could be a cancerous area of over 50 mm that has spread to 1-3 axillary lymph nodes. For the second phase of Stage III (Stage IIIB), the cancer may have been diagnosed as Inflammatory Breast Cancer due to its spread to the chest wall, swelling, and ulceration of the breast. Sometimes it will have spread to 9 or more lymph nodes–again, mammary or axillary–but most likely nowhere else. In Stage IIIC, any tumor will have spread to 10 or more lymph nodes. These could be mammary lymph nodes, axillary lymph nodes, or the lymph nodes under the collarbone. However, the cancer still has not spread throughout the body.
Stage IV is also known as Metastatic cancer. Metastasis is when the cancer has spread to other parts of the body such as distant lymph nodes, bones, other organs, or the chest wall. The tumor can be any size. Cancer is first diagnosed as metastatic about 5-6% of the time and is most commonly found after previous diagnoses of early breast cancer.
Survival Rate of Invasive Ductal Carcinoma
As of 2017, the survival rates for people treated for breast cancers have been increasingly favorable. For those in stages zero and one, the survival rate–measured as the five-year survival rate–is nearly one hundred percent. For those with stage two breast cancer, the survival rate is 93 percent, an increase from the 86 percent survival rate of 2014. For stage three, the five-year survival rate is 72 percent, a dramatic increase from 2014’s 57 percent. Finally, stage four is currently holding at a 22 percent survival rate, a jump from 2014’s 20 percent.
Is Invasive Ductal Carcinoma Curable?
Just as every patient’s experience with cancer is unique, so is their treatment. There may be a form of drug therapy, such as chemotherapy, a hormone therapy, HER2 targeted drug, or some combination. There could be surgery such as a breast-conserving surgery (lumpectomies, partial mastectomies) or a mastectomy, which can involve breast reconstruction. The patient may need radiation therapy to prevent a recurrence of the cancer. Your treatment route is determined by many factors. Family history can come into play, as can the size of the cancer, the type of tumor, maybe genetics, and how far this invasive breast cancer has spread. However, just as important is you and where you stand in all the chaos. Make sure you understand what your treatments are. Ask your doctors questions. They are there to assist you through your process and make sure you are receiving the right treatment.
Dr. Valerie Gorman
Dr. Gorman and everyone with her at the Texas Breast Center are there to help you with your questions about invasive ductal carcinoma and its treatment. She will walk with you through the whole process, and she knows how important it is for you to be informed. She and her team will cater your treatment to your needs and walk with you on your journey through this process.
Breast surgeon Dr. Valerie Gorman presented at the Annual Meeting of the American Society of Breast Surgeons. Hologic, Inc. (Nasdaq: HOLX) will showcase its growing breast surgery franchise, which includes products such as the new Trident® HD specimen radiography system, LOCalizer ™ wire-free guidance system and the BioZorb ® marker, in Booth #103 at the 20th Annual Meeting of The American Society of Breast Surgeons (ASBS) in Dallas from April 30 to May 5.
The pioneer behind the Genius™ 3D Mammography™ exam, Hologic has recently expanded its product portfolio significantly through insight-driven innovation and strategic acquisitions to address the entire clinical continuum of breast cancer diagnosis and care. From digital specimen radiography and stereotactic breast biopsy systems to breast biopsy markers and surgical guidance systems – Hologic’s comprehensive suite of products is designed to meet the unmet and changing needs of radiologists, pathologists and breast surgeons.
“ASBS marks an exciting milestone this year as we debut our newly expanded portfolio of breast-conserving surgery solutions,” said Pete Valenti, Hologic’s Division President, Breast and Skeletal Health Solutions. “We look forward to building upon our relationships with this community of leading breast surgeons and showcasing our growing suite of products designed to improve cancer detection, patient satisfaction and comfort, and facility workflow.”
Hologic Products
A sampling of the products on display in the Hologic booth includes:
The Trident®HD specimen radiography system, a next-generation solution that delivers enhanced image quality, improved workflow, and instant sample verification during breast-conserving surgeries and stereotactic breast biopsies. 1 The system, which recently received FDA clearance in the U.S. and a CE Mark in Europe, uses amorphous selenium direct capture imaging – the same detector technology used in Hologic’s 3Dimensions™ mammography system – to generate crisp, clear, high-resolution images. The system also features a bigger detector that allows for complete imaging of larger breast surgical specimens, along with a wide range of surgical and biopsy samples. 2
The LOCalizer™wire-free guidance system, which is designed to enable precision and ease of use for breast surgery guidance. The LOCalizer tag is designed to replace traditional wire-guided methods, helping provide increased comfort and convenience for patients and their healthcare teams. Additionally, the Tag is designed to be implanted into the breast any time prior to the surgery, providing increased flexibility for patients and providers. A recent study has shown that the LOCalizer tag may be able to reduce positive margin rates with lumpectomy due to the unique feature of reading distance from the tag. 3
The BioZorb®3D bioabsorbable marker, an implantable three-dimensional marker that potentially enables a more targeted radiation therapy and helps clinicians overcome challenges in breast-conserving surgery or lumpectomy. When used to mark the surgical site, BioZorb has been shown to yield good to excellent cosmetic outcomes for at least two years post-surgery and result in minimal scarring on mammography after breast-conserving surgery. 4,5 Additionally, the marker has been shown to improve accuracy in setup and boost targeting as reported by 96 percent of radiation oncologists. 6
The TruNode®wireless gamma probe, a sterile, single-use device for common, radio-guided surgical procedures that senses hotspots using an innovative detector and heuristic audio feedback technology. The TruNode probe is designed to perform less invasively and may reduce infection risk from reprocessing due to its sterile, single-use performance.
Dr. Gorman’s Presentation on 5-day Radiation Therapy
Hologic will also host a breakfast symposium, BioZorb® and a New Way to 5-day radiation, featuring Cary Kaufman, MD, FACS and Valerie Gorman, MD, FACS on Saturday, May 4 from 6:30 – 7:45 am. Additional hands-on workshops hosted by Hologic will cover topics such as stereotactic breast biopsy, oncoplastic skills, and portable breast ultrasound.
The Genius ™ 3D Mammography ™ exam (also known as the Genius ™ exam) is only available on a Hologic® 3D Mammography™ system. It consists of a 2D and 3D ™ image set, where the 2D image can be either an acquired 2D image or a 2D image generated from the 3D ™ image set. There are more than 6,000 Hologic 3D Mammography ™ systems in use in the U.S. alone, so women have convenient access to the Genius exam. To learn more about the Genius exam, visit http://www.Genius3DNearMe.com.
About Hologic, Inc.
Hologic, Inc. is an innovative medical technology company primarily focused on improving women’s health and well-being through early detection and treatment. For more information on Hologic, visit www.hologic.com.
Hologic, 3D, 3D Mammography, 3Dimensions, BioZorb, Genius, The Science of Sure, Trident and TruNode are trademarks and/or registered trademarks of Hologic, Inc., and/or its subsidiaries in the United States and/or other countries. Hologic is an exclusive distributor and licensee of the LOCalizer product and trademark, which is manufactured by Health Beacons.
Forward-Looking Statements
This news release may contain forward-looking information that involves risks and uncertainties, including statements about the use of Hologic products. There can be no assurance these products will achieve the benefits described herein or that such benefits will be replicated in any particular manner with respect to an individual patient, as the actual effect of the use of the products can only be determined on a case-by-case basis. In addition, there can be no assurance that these products will be commercially successful or achieve any expected level of sales. Hologic expressly disclaims any obligation or undertaking to release publicly any updates or revisions to any such statements presented herein to reflect any change in expectations or any change in events, conditions or circumstances on which any such data or statements are based.
This information is not intended as a product solicitation or promotion where such activities are prohibited. For specific information on what products are available for sale in a particular country, please contact a local Hologic sales representative or write to [email protected].
SOURCE: Hologic, Inc., used by permission.
1 Wilson A. Trident 2.0 QUAL Qualitative Findings. Explore and identify the ideal breast biopsy verification system from the OR. Kadence International. July 2016.
2 Compared to original Trident system
3 N = 50 patient, single arm pilot study. DiNome M et al. Microchipping the breast: an effective new technology for localizing non-palpable breast lesions for surgery. Poster presentation, Society of Surgical Oncology annual meeting, Mar 27-30, 2019.
4 Kaufman, et al. Oncoplastic Surgery with the 3-D Tissue Implant Maintains Post-Lumpectomy Breast Contour. Poster presented at the American Society of Breast Surgeons 18th Annual Meeting, May 2-5, 2018.
5 Kaufman CS, et al. Registry Study of 337 Bio-Absorbable 3-D Implants Marking Lumpectomy Cavity Benefit Cosmesis While Targeting Radiation. Poster presented at the Society of Surgical Oncology Annual Cancer Conference March 15-17, 2017.
6 Harms S, et al. Mammographic imaging after partial breast reconstruction: Impact of a bioabsorbable breast implant. J Clin Oncol 33, 2015 (suppl 28S; abstr 111)
View source version on businesswire.com:https://www.businesswire.com/news/home/20190430005179/en/
Simple/Total Mastectomy–The entire breast is removed; lymph nodes and muscle are not removed.
Radical Mastectomy–The entire breast is removed, this time including the pectoral muscles and lymph nodes extending under the arm. This is rarely done today.
Modified Radical Mastectomy–Removes the entire breast including the lymph nodes;
Double Mastectomy–Both breasts are removed.
Lumpectomy/Partial Mastectomy–Part of the breast is removed, namely abnormal tissue or cancer, rather than the whole breast, just removing the lump.
Nipple-Sparing Mastectomy–The breast tissue is removed, but the nipple and skin are left unscathed.
Skin-Sparing Mastectomy–The skin is left intact while the breast tissue, areola, and nipple are removed.
Mastectomies are recommended for those who have large tumors or tumors that affect multiple areas of the breast. They can also be used as a preventative measure for those who carry the BRCA1 or BRCA2 gene or other genetic mutations that increase your risk of breast cancer. The skin- and nipple-sparing mastectomies are newer surgeries. These are optimal for minimal scarring and reconstruction.
What is recovery like for a mastectomy?
Your stay in the hospital after a mastectomy will vary depending on the kind of mastectomy you had, your reactions to the anesthesia, and whether or not you had reconstruction done at the time. However, it can be guaranteed that after surgery, you will be taken to a recovery room until the nurses are sure you are stable and (mostly) alert. At this point, you will be wheeled along to your hospital room where you will stay approximately 1-2 days.
Then, once you are home, you must keep the incisions clean. Your surgeon will give you instructions on how to do so, as well as how to care for your drainage tube, which you will only have with you until your follow up exam.
Your doctor should prescribe you medication for your pain, though the levels vary depending on the location, type of mastectomy, and amount of tissue taken. Follow your doctor’s instructions for approved medication intake.
It usually only takes a few weeks to be back to normal activities, though anything that uses your arms a lot or seems strenuous to your body should be approached cautiously for a while. If you’re ever unsure, you can always check with your doctor. It’s better to be safe than sorry. But soon enough you’ll be back on your feet and facing the world again.
What are mastectomy recovery tools?
While you are recovering, there will be many things you will have directly on your mind. There will be drains to empty and keep untangled, pain medications and antibiotics to keep track of, what will be waiting at home after your stay in the hospital, and your life at large to consider. But there are some tools to help you stay comfortable while you heal. And some people have been patients before you. They have tips to recommend based on their experience.
Some tools that many find helpful are drain belts or robes and mastectomy pillows. There are variations on both of these tools, but both offer support and work to simplify your recovery.
After the mastectomy, drains are left in the area to allow any access fluid to leave the body rather than pooling. The fluid follows a tube to a bulb that you empty regularly and record the amount in them. However, the tubes can quickly become an inconvenience with a risk of snagging. The easiest solution is to attach the drains to your clothes with the velcro attachment or clip them onto a lanyard. But other people have come up with more comfortable and convenient solutions. There are now drain belts, which are comfortable belts with holster-like pockets in which the bulbs can sit. There are drain robes that have pockets to keep the drains out of your way. And some companies produce adhesive pockets that will attach to whatever clothes you wear, making your pajamas into drain holders. Dr. Gorman’s surgical team will provide a bra for you post-operatively that includes rings to which you can attach your drains.
Mastectomy pillows are pillows that are shaped or placed in a way to help support you after your surgery. This can be anything from a regular pillow that is placed under your knees to raise your legs and increase blood flow to the armpit pillow–a rectangular pillow that lays over your chest with notches cut out for your arms. Some provide support for both breasts, while others go between the breast tissue of one breast and the other. Find the pillow that minimizes pain and discomfort and offers the support and comfort you will need. Volunteers in our community sew rectangular post-op pillows for Dr. Gorman’s patients. Each of Dr. Gorman’s patients receives one of these pillows in recovery immediately after surgery.
Previous breast cancer patients have made suggestions to make your recovery as easy as possible. First, stock up on food—at least two weeks’ worth–before your surgery. You will not want to go shopping while you are healing. And while you may not want to eat right away, you should try to find something light on the stomach so you can take it with your pain medication, such as yogurt or pudding.
When you take your first shower about two days after your surgery—or when Dr. Gorman clears you to do so—it’s generally best to do so sitting in a shower chair. You have been off of your feet and on medication since your mastectomy. It’s safest to sit while you clean yourself off.
Avoid housework. Think of this as an excuse to avoid your chores for as long as you can. You need to heal before you start expending that kind of effort. Similarly, don’t try to rush back to work. Many women recommend waiting at least three weeks before returning to your job. Returning too quickly could not only tire you out but could potentially cause complications. This advice is especially relevant to those who have reconstruction surgery, as well.
Dr. Gorman’s team provides a one-on-one education time for each patient that covers all of this information and more prior to a mastectomy.
What will my mastectomy scars look like?
The type or amount of scarring will differ based on the type of mastectomy you are having done. The total, radical, and modified radical mastectomies will leave a visibly large scar as a large amount of tissue/skin is removed. However, with partial/lumpectomies, skin-sparing, and nipple-sparing mastectomies, the scars are less noticeable. Skin-sparing mastectomies tend to leave behind a scar that is usually where the nipple was previously. The scar of the lumpectomy is small and linear and tends to be hidden away in the crease or around the nipple to avoid detection. Lastly, the nipple-sparing mastectomy generally leaves a scar under the breast, where it can be tucked away in the bra-line to avoid visibility.
The Texas Breast Center utilizes Hidden Scar™ Breast Cancer Surgery to help minimalize scarring in patients. Dr. Gorman works with each patient to make the right decision for them on the right kind of mastectomy, and from there to ensure the scarring will be minimal and where it will as minimally intrusive as possible.
How does breast reconstruction work?
Not everyone has breast reconstruction after a mastectomy. For example, those having lumpectomies do not necessarily need one, because a majority of the breast tissue is left alone in the breast. With a mastectomy, reconstruction is more likely as all the tissue was removed. However, it really is up to the patient. Talk to your surgeon about your preferences so that they can be informed when discussing your options with you
What are the risks of a mastectomy?
A mastectomy, like any other surgery, has its risks. There will be swelling in the area, as well as bruising for a while after the surgery. The breast will be sore and scar tissue will form and likely harden. Some patients experience phantom pain in removed breasts. More seriously, however, the incisions could bleed or become infected, or, more rarely, skin necrosis. There is a risk of lymphedema or swelling in the arm where lymph nodes were removed. Seromas (fluid filling the now-empty breast) can form. And not the least of the risks can be a change in self-confidence.
Dr. Gorman is aware of these risks and is there to help prevent them. If they can’t be avoided, she will support you through them and work with you on a plan to improve, step by step.
Should I have radiation or chemo with my mastectomy?
Chemotherapy is not used in all cases of breast cancer. And, if it is used, it is not always used in the same way. There are two primary ways it is used concerning surgery.
Some kinds of chemotherapy–neoadjuvant chemotherapy–is used before surgery as an attempt to shrink the tumor to a more manageable size that requires less extensive surgery. Adjuvant chemotherapy is given after surgery to kill any possible remaining circulating cells that may have been left behind to prevent more tumor growth.
Radiation is often recommended after a mastectomy as a tool to prevent the recurrence of cancerous growth. Traditionally, radiation is administered for five to six weeks, up to five days a week. However, Dr. Gorman has experience with a method that only takes five days, with less waiting period between surgery and the radiation beginning for post-lumpectomy patients.
Can men get a mastectomy?
Breast cancer in men may be rare, but it is still very possible. Only 1% of breast cancer diagnoses are in men, but that still accounts for 1 in every 1,000 men. Invasive Ductal Carcinoma is the most common form of breast cancer found in men. Like in women, black men have a higher risk of getting breast cancer than those of other races. Take precautions and familiarize yourself with the breast area by firmly feeling over the breast tissue in the area for anything unusual.
If a man receives a diagnosis for breast cancer, there is a high chance surgery will be involved in treatment. The operation could be used to establish how far into the lymph nodes the cancer has spread (a sentinel lymph node biopsy, for example), to relieve symptoms of advanced cancer, or to remove as much of the tumor itself as possible (a mastectomy).
All of these and a few more can be performed on a man to help treat him for breast cancer. It is not just women who get this disease, and today’s treatments reflect that.
How do I take blood pressure after a mastectomy?
There is some question about where to have blood pressure taken and blood drawn from post-mastectomy; more specifically, patients ask whether it is safe to do these things on the same side of the body as the mastectomy. While you can have your blood pressure tested from either arm without causing any trouble to your healing process, there could be a (minimal) risk when it comes to drawing blood after breast cancer surgery.
After certain types of mastectomies–radical mastectomy, modified radical mastectomy, sentinel lymph biopsy, or any procedure when the lymph nodes are removed–there is a risk of lymphedema. Lymphedema is a swelling of the arm and usually stems from an infection of the arm. Because having blood drawn in a medical facility is done in a clinical environment with sterile equipment, the already small risk of infection becomes minimal. However, it is still recommended to take the ‘better safe than sorry’ route and instead have your blood drawn from the arm opposite your operation.
The same goes for vaccines and other injections. While the medication won’t cause any complications, it’s best to reduce the chances of introducing possible infections to the area soon after your breast surgery or years later.
What do I ask my surgeon?
You should always prepare a few questions when going into a procedure like this. Likely, a number of them will get answered simply through the surgeon’s explanation of the process, but it never hurts to be prepared. Here a few to get you started:
What are the risks of my type of mastectomy?
Will I need reconstruction? Can it be done in the same procedure?
How can I prepare my home for my recovery before the procedure?
How can I emotionally prepare for this?
What medicines/foods should I or shouldn’t I take on the day of the procedure?
Who will perform my breast reconstruction surgery?
How much breast tissue will be removed in my mastectomy?
Will I need radiation therapy?
How long will I stay in the hospital?
Will I need to return for additional surgery?
And remember, there really are no stupid questions. None. This is your surgery, you deserve to know about it, and Dr. Gorman is here to help you understand. Ask away and she will do her best to answer. She will help with your before questions, your after questions, and your it’s-been-a-while-but-this-just-occurred-to-me questions. Being informed is something she wants for all of her patients, and something she will do her best to ensure as she walks with you every step of the way.
Who performs a mastectomy?
A breast cancer surgeon will perform your mastectomy, and a plastic surgeon will perform your breast reconstruction should you have that done. When choosing your surgeon, Johns Hopkins recommends a surgeon who:
Specializes in breast cancer
Is recognized as a breast surgical oncologist
Performs many breast cancer surgeries each year
Looking at these qualifications, Dr. Valerie Gorman at the Texas Breast Center can be your breast cancer surgeon, and of course, is always ready to help. Her specialty is breast cancer surgery and its related topics. Her residency was in general surgery, though with a focus on detecting and treating breast cancer. She is also currently serving as the Chief of Surgery and Medical Director of Surgical Services at Baylor Scott & White Medical Center, as well as board-certified by the American Board of Surgery.
At the Texas Breast Center, mastectomies and other breast cancer surgeries are what Dr. Gorman is known for, and she performs them year-round.